October 2013–September 2014

Many countries have acknowledged community‐based infant and young child feeding (IYCF) promotion, counseling, and support as one of the key pillars of IYCF strategies. In 2009, the United Nations Children’s Fund (UNICEF) and the World Health Organization (WHO) agreed that a global, generic IYCF training package for community health workers was needed to complement the WHO/UNICEF Breastfeeding, Complementary Feeding and Infant and Young Child Feeding Integrated Counselling training package, which was specifically designed for facility health workers.
UNICEF committed to leading the development of the proposed response. The UNICEF Community Infant and Young Child Feeding (C‐IYCF) Counselling Package was finalized and field tested under a strategic collaboration between UNICEF New York and the combined technical and graphics team of the Nutrition Policy and Practice (NPP) and the Center for Human Services, the not‐for‐profit affiliate of University Research Co., LLC (URC/CHS). The first edition of the C‐IYCF Counselling Package was published at the end of 2010 and was updated in 2012.
The C‐IYCF Counselling Package, a generic resource, enables community volunteers (CV) and primary health care staff to support mothers, fathers, and other caregivers to optimally feed their infants and young children.
The training component of the package ensures that CVs have the knowledge and expertise they need by—
- teaching them the recommended breastfeeding and complementary feeding practices for children from 0 to 24 months
- honing their group facilitation, interpersonal communication, counseling, problem solving, and negotiation skills
- preparing them to use the related counseling tools and job aids effectively.
The various elements of the C‐IYCF Counselling Package are based on WHO/UNICEF IYCF guidance documents, training, and other materials; including the WHO/UNICEF Breastfeeding, Complementary Feeding and Infant and Young Child Feeding Integrated Counselling training courses. The package also builds on materials developed by the Academy for Educational Development’s LINKAGES Project; the CARE USA and URC/CHS collaboration in Dadaab Kenya; and the Integration of IYCF Support into Community Management of Acute Malnutrition (CMAM), produced by the Emergency Nutrition Network (ENN)/ Infant Feeding in Emergencies (IFE) Core Group and Inter‐Agency Standing Committee (IASC) Global Nutrition Cluster. The technical content of the package aims to reflect the Guidelines on HIV and Infant Feeding 2010: Principles and Recommendations for Infant Feeding in the Context of HIV and a Summary of Evidence, related to IYCF, in the HIV context.
The package includes specific guidance for adapting it at the country level, especially aspects related to the development of messages that target cultural barriers to optimal breastfeeding and complementary feeding practices. Guidance and tools for data collection, monitoring, quality assurance and supervision, as well as guidance and tools for developing contextually appropriate local graphics for training aids and counseling material are also included—essential elements intended to ensure an effective, sustained, and quality program. To date, some 30 countries are at various stages of adapting the C‐IYCF Counselling Package to the local context, building capacity, and rolling out community‐based IYCF programming.
Study Rationale and Objectives
Despite the global interest in the C‐IYCF Counselling Package, very little is known about its impact on IYCF behaviors in the countries where it has been adapted. For this reason, high‐quality studies are needed. Nigeria offers a unique opportunity to address this major gap in global evidence because the Federal Ministry of Health (FMOH), with support from two USAID‐funded global nutrition projects—IYCN and Strengthening Partnerships, Results and Innovations in Nutrition Globally (SPRING)—has made a significant investment in adapting the generic C‐IYCF Counselling Package to the Nigerian context, including its translation into six local languages. Nigeria has committed to a national rollout of the C‐IYCF program, starting in several Nigerian states where funding is secured. After consultations with both SPRING and UNICEF, the FMOH agreed to evaluate the package, knowing that the findings—which will be shared both nationally and internationally—will inform future investments in C‐IYCF programming.1
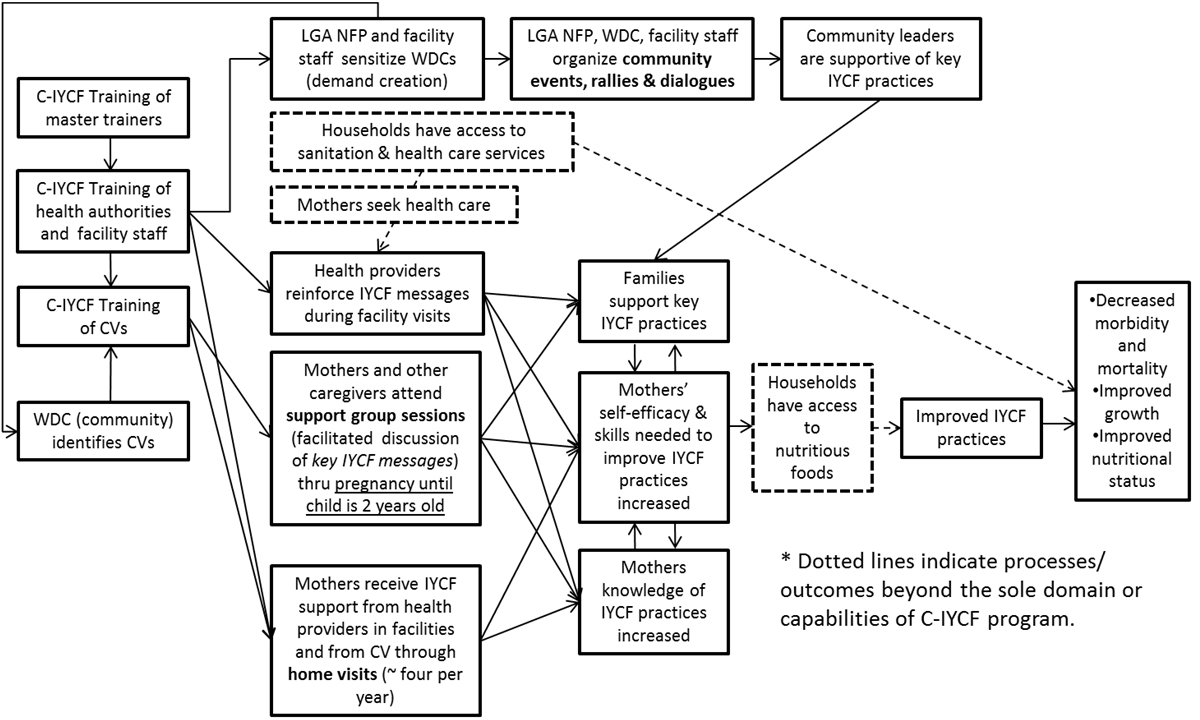
The study’s main purpose is to assess the effectiveness of the C‐IYCF Counselling Package, which has been adapted for the local context and implemented at scale2 in an environment that supports its design, management, technical assistance, and monitoring. The results from this study will make an important scientific contribution to the field of nutrition, which has relatively little evidence on the impact of a large‐scale community‐based IYCF counseling intervention. See figure 1.
The objectives of the study are to—
- Assess the environment or context in terms of how it either “enabled” or hampered the success of the implementation of the C‐IYCF program in Kaduna state, Nigeria.
- Assess the planning, processes, and costs of the C‐IYCF Counselling Package.
- Evaluate the outcomes of implementation of the C‐IYCF Counselling Package on counseling and communication skills and knowledge of IYCF among CVs.
- Determine the impact of implementation of the C‐IYCF Counselling Package on caregivers’ knowledge, attitudes, beliefs, and practices related to IYCF.
Figure 1: C‐IYCF Program Impact Pathways
Study Location
The study will be conducted in one intervention local government area (LGA) and one comparison LGA in the state of Kaduna.3 The FMOH plans to implement C‐IYCF in the comparison LGA after this study has been completed. The intervention LGA will be Kajuru and the comparison LGA will be Kauru, which was selected because its socio‐demographic characteristics are most similar to the intervention LGA. In addition, data from key informants will be collected at the national level in the Federal Capital Territory and state level in the Kaduna LGA (Kaduna’s state capital).
Study Design

The study will follow a quasi‐experimental design using a mixed‐method approach for answering the research questions. After 18 months of program implementation— using a number of different data collection methods described below—quantitative and qualitative data will be collected at the baseline and, again, at endline. While the facility assessment, the semistructured interviews, as well as the survey of CVs and health workers, will be longitudinal (i.e., every attempt will be made to follow the same individuals at baseline and endline), the maternal survey will capture repeated cross‐sectional samples of pregnant women and mothers/caregivers of children under 2 years old. A slide deck on the study protocol is included in annex 1.
Intervention
After baseline data are collected, the C‐IYCF program will be implemented by the Kaduna State Ministry of Health (SMOH), with support from UNICEF/Nigeria. UNICEF will cover the cost of trainings, as well as snacks and transportation to and from meetings. The intervention will be implemented with minimal outside funding, building on established health and community systems. The package has been rolled out similarly in many countries. SPRING and UNICEF believe that such an approach increases scalability and sustainability. See annex 1 for additional details on plans for program implementation.
Progress to Date
The planning and design of this activity began in the fall of 2013, beginning after SPRING, UNICEF New York, and UNICEF Nigeria established a partnership. In March 2014, SPRING contracted a principal investigator, Rafael Perez‐Escamilla. To define the roles and responsibilities among partners, we held a number of stakeholder meetings were in Nigeria, in person, and by phone. In April, we developed a draft protocol and circulated it for review. In May, the co‐principal investigator, Sascha Lamstein, planned to travel to Nigeria to hire a local study coordinator and launch the study. However, because of an increased security risk following several attacks by Boko Harem, and in anticipation of the World Economic Forum on Africa meeting, we postponed the trip until July.
Between June and September 2014, with input from UNICEF, SPRING finalized the study protocol and numerous data collection tools, and completed the recruitment process for a local study coordinator. In addition, SPRING worked closely with UNICEF to develop a detailed implementation plan for the C‐IYCF counseling program in Kajuru LGA, Kaduna state.
SPRING offered the position of study coordinator to the top candidate. Unfortunately, this person declined. A new candidate, who is available immediately, was interviewed and reference checks are underway.
In addition, SPRING solicited approval from JSI’s Institutional Review Board (IRB) to proceed with the study.
Next Steps
In the near future, SPRING will finalize recruitment of the study coordinator.
In preparation for baseline data collection, SPRING will submit necessary documentation to the National Health Research Ethics Committee of Nigeria (NHREC) in October 2014 for in‐country ethical review and approval. UNICEF will then contract the firm(s) for data collection, which will begin in late 2014.
UNICEF/Nigeria, in collaboration with UNICEF/Kaduna and the SMOH, will review and finalize implementation plans in the fall of 2014. Implementation activities will begin in 2015 and the SMOH and UNICEF will lead them. The first step in implementation will be to sensitize the SMOH, LGA, and Ward Development Committees to ensure they understand the roles and commitments for identifying eligible health facilities, health facility staff, and CVs; training of health authorities, health facility staff, and CVs; sensitization of communities through rallies and events; and supportive supervision/mentoring and monitoring.
Footnotes
1 The Principal Investigators (PI) of this evaluation are Rafael Perez-Escamilla of Yale University, consultant to SPRING, and Sascha Lamstein of SPRING. The co-investigators include Peggy-Koniz-Booher (SPRING), France Begin (UNICEF), Arjan De Wagt (UNICEF), Christine Kaligirwa (UNICEF), Babajide Adebisi (SPRING), and Chris Isokpunwu (FMOH). In addition, this work would not have been possible without the the support of Stanley Chitekwe, Davis Omotola, and Florence Oni of UNICEF, and the efforts of Susan Adeyemi, Emily Stammer, and Sarah Cunningham of SPRING.
2 Note that “scale” is defined as an LGA, a geographic area and population considered adequate for assessing replicability and generalizability to implementation at the national level.
3 We considered comparing government-led implementation of the package to implementation led by international nongovernmental organizations. However, ensuring the validity and rigor of such a study would require a high level of control for each study arm, which was not possible.