Executive Summary
Introduction
Despite significant progress toward improving health outcomes, Senegal continues to face challenges around optimal nutrition, especially for women and children. Twenty-one percent of Senegalese children under five are stunted, a measurement of chronic undernutrition (Agence Nationale de la Statistique et de la Démographie (ANSD) [Sénégal] & ICF 2016). Only 33 percent of Senegalese infants are exclusively breastfed during the first six months and, in rural areas, a mere 10 percent of children 6–23 months receive a minimum acceptable diet (MAD) (Agence Nationale de la Statistique et de la Démographie (ANSD) [Sénégal] & ICF 2016). Lack of access to affordable, nutrient-dense foods from animals and horticulture is a barrier to good nutrition; poor hygiene practices also contribute to stunting. These conditions can lead to high prevalence of gastrointestinal illnesses that contribute to undernutrition (Black et al. 2008). At the request of the U. S. Agency for International Development (USAID) Mission in Senegal, the Strengthening Partnerships, Results, and Innovations in Nutrition Globally (SPRING) project established a presence in the country in November 2015 with a goal to improve nutrition among households in the project Zone of Influence (ZOI) by increasing coverage of the optimal package of nutrition-sensitive and nutrition-specific interventions.
SPRING’s package of interventions, which centered on working with agricultural networks to increase demand for and access to key inputs and services to support nutrition-sensitive agriculture, included a robust community media approach to increase awareness of and demand for good nutrition-related practices and services. Specifically, SPRING worked with local communications and media partners to create informative, engaging, and culturally appropriate content on nutrition- and hygiene-related practices and disseminate this information to communities within the ZOI. In addition to using community radio to promote desired behaviors, SPRING and its partner Digital Green (DG) introduced an innovative community video approach to leverage local experiences and create highly contextualized videos that promote a variety of multi-sectoral nutrition-specific and nutrition-sensitive behaviors.
This report presents findings from a quantitative study assessing the effectiveness of SPRING/DG’s community media approach and the value of the community video intervention for improving nutrition and hygiene behaviors in Senegal.
Research Questions
The study aimed to answer the following research questions:
- How do community videos and radio programs influence the knowledge and practices related to nutrition and hygiene in women with children ages 6-23 months?
- What is the added value of implementing community videos and radio programming, as compared to the effect of hearing messages through radio alone?
- What is the added value of implementing the gold standard for community video rollout, i.e. community videos with follow-up home visits, as opposed to not including home visits (which can be time and resource intensive)?
Methods
We used a pre-post quasi-experimental study design with comparison to assess the effectiveness of the community video intervention. We administered cross-sectional surveys at two points in time: a baseline survey prior to video exposure and an endline survey 10 months later, after the rollout of the radio and community video interventions. The sample included 30 villages in SPRING’s ZOI: 10 villages received the community video intervention with follow-up home visits, in addition to SPRING-supported community radio programming; 10 villages received the community video intervention without follow-up home visits and radio programming; and the final 10 villages received community radio programming only.
Results
Breastfeeding
Survey findings show that both community radio and community video were effective in improving knowledge about breastfeeding, but an improvement in the actual practice of early breastfeeding initiation was only seen in the villages where SPRING implemented community video. Specifically, a statistically significant increase in knowledge was noted in both intervention and control villages at endline, leading to a nearly universal understanding of colostrum’s benefits amongst women. Similarly, the intervention and control villages had comparable rates of (self-reported) practice concerning early breastfeeding initiation at baseline. At endline, however, we saw no improvement in the control villages, but a significant increase from 65.4 percent to 86.1 percent in the intervention villages.
Minimum Acceptable Diet
Results indicate that community radio and community video were associated with statistically significant increases in MAD for children ages 6-23 months, though the increase in the intervention villages (11.8 percent at baseline to 61.8 percent at endline) was more than twice that seen in the control villages (16.2 percent to 34.6 percent).
Eating from a Separate Plate
Study findings indicate that community radio was somewhat effective in improving the practice of feeding children from a separate plate, while community video was effective in improving knowledge and practice for this indicator. Following exposure to radio and community video, we observed no significant increase among women who agreed that children should be fed from a separate plate in the control villages, but statistically significant increases to a near universal rate in the intervention villages. In terms of the practice of feeding children from a separate plate, we observed an increase in self-reported behavior in both groups, but this difference was much larger in the villages that received the community video intervention. Specifically, while the percentage of women who fed their child from a separate plate during the last meal increased from 62.7 percent to 73.7 percent in the control villages, it increased from 54.4 percent to 90.2 percent in the intervention villages.
Handwashing
Results for handwashing were mixed but ultimately demonstrate that community videos were effective in promoting the installation of tippy taps in intervention villages. Survey findings indicate that the percentage of women who knew at least one critical moment for handwashing decreased in the control villages and stayed the same in the intervention villages at endline. While we found virtually no fixed handwashing stations in intervention or control villages at baseline, 41 percent of the intervention households had handwashing stations at endline, the vast majority of which were tippy taps. No improvement was seen in the control villages.
Conclusion
Our findings show that community video is an exciting, feasible, and effective social and behavior change communication (SBCC) approach that has the power to change social norms and behaviors. Our experience in Senegal demonstrates the effectiveness of community video in changing nutrition- and hygiene related behaviors, even without follow-up visits. Participants learned and retained many of the key messages shared in the videos by attending a screening of the films and engaging in a facilitated group discussion, without the additional benefit of follow-up home visits. We were unable to conduct the quantitative analysis comparing the effectiveness of this less expensive and more scalable approach with the gold standard approach that includes follow-up home visits, due to difficulties in properly scaling home visits. Despite this, we consider the fact that disseminators were unsuccessful in conducting household visits among at least 50 percent of the target homes a telling finding. For projects that utilize volunteer mediators, as is the case in Senegal, the time opportunity cost for conducting home visits may be too high to scale or sustain, and this simpler approach may provide a more practical option where time and budget constraints are significant. Last, our results show that radio is an excellent way to share information broadly and begin to catalyze change through targeted messages. The addition of community video, as a more direct communication channel, enhances results by reinforcing key messages heard elsewhere.
Introduction
Despite significant advancements to improve health outcomes, Senegal continues to face challenges related to optimal nutrition, especially for women and children. Twenty-one percent of Senegalese children under five are stunted, a measurement of chronic undernutrition (Agence Nationale de la Statistique et de la Démographie (ANSD) [Sénégal] & ICF 2016). Only 33 percent of infants are exclusively breastfed during the first six months and, in rural areas, a mere 10 percent of children 6–23 months receive a minimum acceptable diet (MAD) (Agence Nationale de la Statistique et de la Démographie (ANSD) [Sénégal] & ICF 2016). Women are often unable to access necessary health information and services. As a result, their health practices are often poor, which can contribute to undernutrition. Lack of access to affordable, nutrient-dense foods from animals and horticulture is a barrier to good nutrition; poor hygiene practices also contribute to stunting (Black et al. 2008). Sixty-two percent of rural households do nothing to ensure their water is safe to drink, and only 31 percent of people wash their hands after defecation (World Bank 2004). These practices can lead to high prevalence of gastrointestinal illnesses that contribute to undernutrition.
Within this context, and at the request of the U.S. Agency for International Development (USAID) in Senegal, the Strengthening Partnerships, Results, and Innovations in Nutrition Globally (SPRING) project established a presence in the country from November 2015 through October 2017. Our goal focused on improving nutrition among households in target areas by increasing coverage of the optimal package of nutrition-sensitive and nutrition-specific interventions. The project’s specific objectives were to (1) increase awareness and demand for good nutrition-related practices and services, and (2) facilitate access to key inputs and services essential for good nutrition.

Community Video in Senegal
SPRING’s package of interventions, which centered on working with agricultural networks to increase demand for, and access to, key inputs and services to support nutrition-sensitive agriculture, included a robust community media approach to increase awareness of, and demand for, good nutrition-related practices and services. We worked with local communications and media partners to create informative, engaging, and culturally appropriate content on nutrition-related practices, and disseminate this information to communities within our intervention areas.
In addition to the more conventional use of community to promote essential nutrition actions and essential hygiene actions, SPRING introduced a community video approach. This approach leveraged local experiences and narratives, while using an innovative dissemination channel to reach large numbers of individuals, and excite, motivate, and empower communities to move toward improved nutrition and health. SPRING’s “Community Video for Nutrition” approach engages communities during the design, production, and dissemination stages to create highly contextualized videos that promote a variety of multi-sectoral nutrition-specific and nutrition-sensitive behaviors. Implemented in collaboration with Digital Green (DG), this innovative format blends technology (using portable pico projectors) with interpersonal communication (including mediated discussion groups and subsequent home visits). Our trained mediators disseminated these locally produced videos to promote optimal nutrition and hygiene practices while also addressing underlying gender considerations. The viewings were followed by lively group discussions and in some cases, follow-up home visits at least two weeks after video dissemination. In line with DG’s approach, community members were selected to star in the videos, creating clear ties to the community and increasing the likelihood that viewers would both identify with the messages and adopt the promoted behaviors.
Between March and August 2017, we implemented the community video approach across 104 villages in Senegal’s Kaolack, Fatick, and Kaffrine regions, making 24,489 contacts with the 10 videos produced. Videos were viewed by a mixed group of individuals in each village, including community leaders, women with children under two years of age, and members of agricultural producer networks. Table 1 shows the full list of community videos that were produced and disseminated in Senegal, including the three that are the focus of this study (breastfeeding, complementary feeding, and handwashing).
Table 1. Comprehensive List of Community Videos Produced and Disseminated in Senegal
| No. | Title of Video |
|---|---|
| 1 | The advantages of orange-flesh sweet potato |
| 2 | The importance of exclusive breastfeeding |
| 3 | Complementary feeding |
| 4 | Diversification of agricultural production |
| 5 | Improved village poultry farming |
| 6 | Critical moments for handwashing |
| 7 | Hygiene in the household |
| 8 | The quality sorting of cereals |
| 9 | The drying and preservation of fruits and vegetables |
| 10 | Gender champions |
Conceptual Framework
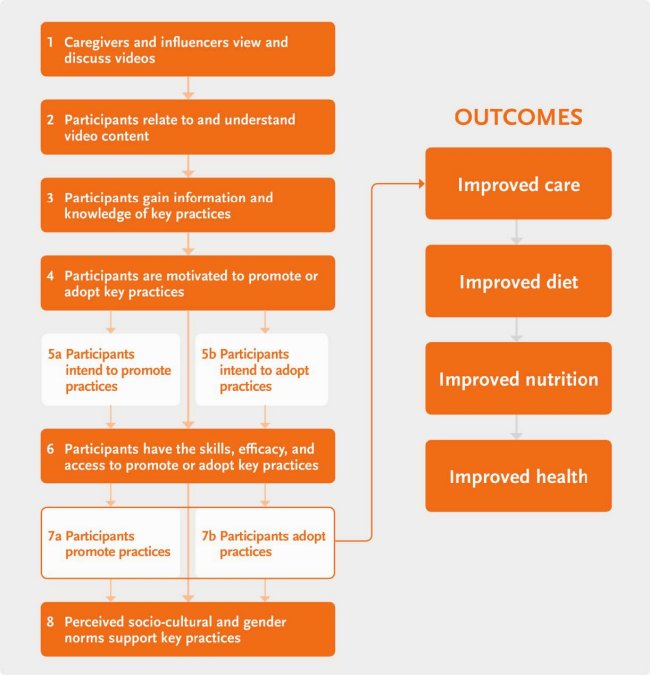
The conceptual framework in Figure 1 shows the SPRING/DG theory of change, which ultimately aims to improve nutrition and hygiene knowledge and practices among the target group, in this case women with children ages 6-23 months. Our community video approach was informed by Bandura’s theory for social learning as well as the socioecological model (Stokols 1996), both of which highlight the importance of addressing the cognitive and behavioral aspects of behavior change. The community video approach seeks to impart nutrition- and hygiene-related knowledge to viewers, thereby addressing the cognitive aspect of behavior change. Moreover, the videos show local community members demonstrating desired behaviors, affirming to viewers that they, too, can achieve the same.
Figure 1. SPRING/DG Senegal Pilot Conceptual Framework
 |
We used a pre-post quasi-experimental study design with comparison to assess the effectiveness of the community video intervention. We administered cross-sectional surveys at two points in time: a baseline survey prior to radio and video exposure and an endline survey 10 months later, after the rollout of the radio and community video interventions. The surveys were designed to determine the effects of rolling out the community media approach in Senegal, by answering the following questions:
- How do community videos and radio programs influence the knowledge and practices related to nutrition and hygiene among women with children ages 6-23 months?
- What is the added value of implementing community videos and radio programming, as compared to the effect of hearing messages through radio alone?
- What is the added value of implementing the gold standard for community video rollout, i.e. community videos with follow-up home visits, as opposed to not including home visits (which can be time and resource intensive)?

A Senegalese boy resting in his mother's arms as she watches during a community video dissemination event.
Methods
| Figure 2. Map of SPRING Study Area in Senegal |
 |
For this study, we selected a sample of thirty villages in the Kaolack and Kaffrine regions, both located within SPRING’s Zone of Influence (ZOI). The villages were in the departments of Kounghuel and Nioro du Rip, in the communes of Ida Mouride and Wack Ngouna, respectively (see Figure 2). Twenty of the 30 villages in the sample benefited from a package of direct SPRING interventions, including community video. These 20 intervention villages fell in two separate categories with respect to the community video rollout: half received the community video intervention without subsequent follow-up home visits, while the remainder benefited from community videos and follow-up home visits conducted by SPRING-trained mediators. The remaining 10 villages were not targeted for any direct SPRING activities and only benefited from hearing SPRING messages through the radio, broadcasted throughout the entire region. The sampling strategy is described in Figure 3.
We used a pre-post quasi-experimental study design with comparison to assess the effectiveness of the community media intervention. We administered cross-sectional surveys at two points in time. The baseline survey was carried out in November 2016, prior to radio and video exposure. The endline was conducted 10 months later, in September 2017, after the rollout of radio throughout the ZOI, and community video in the 20 intervention villages.
| Figure 3. Sampling Strategy |
 |
To address the outcomes of interest, we targeted women of reproductive age (15-49 years) who, at baseline, had at least one child ages 6-23 months. All women who met these criteria and lived in the 30 study villages were eligible for inclusion. The endline was comprised of all women interviewed at baseline (even if the child was over the age of 23 months by that time) and included additional women whose children entered the 6 to 23 month age range over the study period. For this reason, the endline sample size (533 women) was larger than the baseline sample (490 women). Despite this expansion in the total sample size at endline, we limited baseline and endline samples to women who had children ages 6-23 months at the time of the survey when calculating the MAD. Similarly, with respect to the practice of early initiation of breastfeeding, which was asked retrospectively in the survey, we limited the endline sample to women who had given birth after the baseline to ensure that they had the opportunity for radio and/or video message exposure.
We collected baseline data with the use of paper-based forms. At endline, we used Survey CTO’s mobile data collection platform to conduct surveys. At baseline, we selected eligible participants with the help of local community health workers (CHWs) and by using a village-level health facility roster. At endline, we pulled baseline participant names from project records to ensure we captured them all. Furthermore, we worked with CHWs to identify additional women who met the criteria for inclusion. At the onset of the interview, data collectors asked questions related to age and date of last birth to confirm eligibility, and only then did the survey proceed. Interviews were conducted in Wolof and recorded in French using paper surveys (at baseline) or mobile tablets (at endline). Supervisors implemented data quality checks on the field and at the end of each day.
The baseline and endline surveys collected information on knowledge and practices promoted through community media that focused on breastfeeding initiation, dietary diversity, responsive feeding, and handwashing. Indicators assessing behaviors, described below, were self-reported except where noted.
Breastfeeding
- Percentage of women who knew the importance of early breastfeeding
- Percentage of children who were breastfed within an hour of being born
Minimum Acceptable Diet
- Percentage of children who received a minimum acceptable diet (MAD) in the previous 24 hours
- Percentage of children who received solid, semi-solid, or soft foods the minimum number of times or more in the previous 24 hours
- Percentage of children who received four or more food groups in the previous 24 hours
Eating from a Separate Plate
- Percentage of women who thought that child should be fed from a separate plate
- Percentage of women who fed child with a separate plate for each meal
Handwashing
- Percentage of women who knew the critical moments for handwashing
- Percentage of households with fixed handwashing station (observed by interviewer)
- Percentage of households with water and soap available at handwashing station (observed by interviewer)
- Percentage of households with a handwashing station near the latrine or the kitchen (observed by interviewer)
All data were managed, cleaned, and analyzed using Stata14. We used bivariate analyses to assess differences in knowledge and practices between baseline and endline. We conducted significance tests and considered results with p-values less than 0.05 statistically significant.
Ethical Considerations
The study protocol and questionnaires were reviewed and approved by John Snow, Inc.’s institutional review board as well as Senegal’s Direction de la Planification de la Recherche et des Statistiques. Participation in the study was voluntary and non-coercive, and we obtained written informed consent from all participants. All participant data were treated as confidential; data were de-identified before being stored and backed up on password-protected file drives. Only members of the evaluation team had access to these data.
Results

In this section, we present results from the surveys by research question, and demonstrate the influence of the community media intervention. We contrast results between intervention and control villages in terms of assessing the effects of radio programming and/or the community video approach on a select number of SPRING-promoted nutrition and hygiene knowledge and practices.
Our third research question focuses on demonstrating the added value of the gold standard—the dissemination of community videos with subsequent home visits—as opposed to a community video only approach. Unfortunately, we were not able to make this comparison using the available data, because home visits were so rare (less than 5 percent of the total sample). We reviewed project records to understand the challenges faced in the scale up of home visits and discovered that mediators, who worked on a volunteer basis to disseminate videos and conduct home visits, found home visits too time-consuming. In comparison to a video viewing session, which extended to a maximum of one hour, a home visit required at least 45 minutes per household. For volunteer mediators who were asked to cover an average of 20 households, the time opportunity cost was simply too high. While unfortunate, these challenges are informative and important to recognize. We have incorporated thoughts on this in the ‘Discussion and Conclusions’ section below.
Breastfeeding
The project’s community video on breastfeeding highlighted the benefits of colostrum for the newborn and emphasized the importance of early breastfeeding. Figures 4 and 5 present women’s knowledge and self-reported practices related to early breastfeeding before and after video exposure, respectively. As shown in Figure 4, baseline findings showed that the majority of women in both intervention and control villages were able to cite at least one of colostrum’s benefits. The knowledge base was comparable across villages in the intervention (86.5 percent) and control (84.8 percent) groups. At endline, a statistically significant increase in knowledge was noted in both intervention and control villages, leading to a nearly universal understanding of colostrum’s benefits amongst women—98.6 percent and 96.0 percent, respectively.
We also asked women about their practices related to early breastfeeding initiation, which we defined as breastfeeding within the first hour of childbirth. As Figure 5 shows, the intervention and control villages had comparable rates of practice at baseline. At endline, we saw a significant increase from 65.4 percent to 86.1 percent in the intervention villages, but no improvement in the control villages. In contrast to women’s knowledge regarding the benefits of colostrum, improvement in practice was only seen in villages where SPRING implemented community video.
Figure 4. Early Breastfeeding: Knowledge of Women with Last-born Child
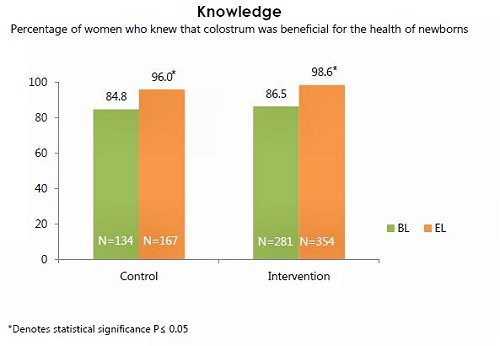
Figure 5. Early Breastfeeding: Practice of Women with Last-born Child

Note: In the survey instrument, the question related to the practice of early breastfeeding initiation was asked retrospectively. Women were asked to think back to the birth of their last child to answer this question. For this reason, we limited the endline study sample to women who had given birth after the baseline. Women who gave birth before the baseline would not have been exposed to the intervention in time to make changes to their practices around early breastfeeding initiation.
Minimum Acceptable Diet
Figure 6 presents self-reported practice data related to MAD for children ages 6-23 months, including results for dietary diversity and meal frequency. While the percentage of children ages 6-23 months who received MAD was low in control villages at baseline, it increased significantly in the endline, from 16.2 percent to 34.6 percent. We saw a more notable increase in the intervention villages, from 11.8 percent at baseline to 61.8 percent at endline.
We investigated individual meal frequency and dietary diversity indicators and noted interesting differences. To gauge practices related to meal frequency, we asked mothers how many times they fed their children ages 6–23 months in the 24 hours preceding the survey. At endline, the percentage of children who received the minimum meal frequency increased from 50.7 percent to 89.0 in the intervention villages—far more sizable than the improvement seen in the control villages, which increased from 53.5 percent to 71.2 percent between the two surveys (see Figure 7). For dietary diversity, we asked women how many food groups they fed their 6-23 month-old children in the 24 hours preceding the survey. The trends were very different: while dietary diversity practices remained largely unchanged in the control villages at endline, we observed a statistically significant increase from 18.3 percent to 63.9 percent in the intervention villages (see Figure 8).
Figure 6. Minimum Acceptable Diet: Practices of Women with a Child Ages 6-23 Months
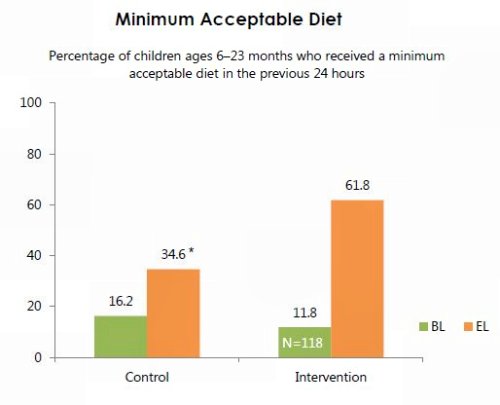
Figure 7. Number of Child Feedings in Previous 24 Hours

Figure 8. Children Who Received Four or More Food Groups in Previous 24 Hours

Note: When computing results for MAD, minimum meal frequency, and minimum dietary diversity, we limited our sample to women who had children between the ages of 6-23 months at the time of the survey. Atlhough the overall endline sample included children from baseline who may have been older than 23 months by endline, these children were not included during the calucation of these indicators.
Eating from a Separate Plate
As shown in Figure 9, we observed high and comparable rates of respondents agreeing that children should be fed from a separate plate at baseline (84.1 percent in the control group and 83.0 percent in the intervention group). Following exposure to community video, which emphasized the importance of feeding children from a separate plate, knowledge among women in the control villages stayed similar, but increased significantly to a near universal rate (96.4 percent) in the intervention villages.
When it came to the practice of feeding children from a separate plate, we observed an increase in self-reported behavior in both groups, but this difference was much larger in the villages that received the community video intervention (see Figure 10). Specifically, the percentage of women who fed their child from a separate plate during the last meal increased from 62.7 percent to 73.7 percent in the control villages, compared to a jump from 54.4 percent to 90.2 percent in the intervention villages.
Figure 9. Use of a Separate Plate: Knowledge of Women with a Child Ages 6-35 Months

Note: The endline was comprised of all women interviewed at baseline, even if the child was over the age of 23 months by that time. For this reason, the endline sample includes children 6 to 35 months.
Figure 10. Use of a Separate Plate: Practice of Women with a Child Ages 6-35 Months

Note: The endline was comprised of all women interviewed at baseline, even if the child was over the age of 23 months by that time. For this reason, the endline sample includes children 6 to 35 months.
Handwashing

We asked women about their knowledge of critical moments for washing hands. Between baseline and endline, the percentage of women who knew at least one critical moment for handwashing decreased in the control villages, while it stayed the same in the intervention villages (see Figure 11). The reduction in knowledge in the control villages and the lack of improvement in the intervention group, despite the emphasis on this topic in community radio and video about handwashing, require further inquiry. In countries like Kyrgyzstan with substantial fluctuations in weather, SPRING has found that seasonal differences can affect people’s desire and likeliness to wash their hands, but this does not seem likely in Senegal.
Figure 11. Handwashing: Knowledge of Critical Moments among Women with a Child Ages 6-35 Months

Note: The endline was comprised of all women interviewed at baseline, even if the child was over the age of 23 months by that time. For this reason, the endline sample includes children 6 to 35 months.
We also checked to see if households had fixed stations for washing hands (tippy taps qualified). At baseline, we found virtually no fixed handwashing stations in intervention or control villages. Instead, women showed us various containers they used for handwashing, but no one had a designated, stationary area for washing hands. At endline, only 2 percent of households in the control villages had a fixed station for handwashing, while 41 percent of the intervention households had handwashing stations. The vast majority of these handwashing stations (97 percent) were tippy taps, a device that was heavily promoted by the SPRING project. As shown in Figure 12, among households with at least one fixed handwashing station, 90 percent and 84 percent had one installed near a latrine and a kitchen, respectively. Additionally, 79 percent of these households also had water and soap by the station.
Figure 12. Location of Handwashing Stations Among Households that Had At Least One Fixed Station in the Intervention Villages at Endline

Discussion and Conclusion
Our experiences have shown that community video is an exciting, feasible, and effective SBCC approach that has the power to change social norms and behaviors. Community video showcased positive role modeling of recommended behaviors to help stimulate behavior change. This innovative storytelling model facilitated learning of new concepts, as well as communication among village peers, to catalyze behavior change. Two principle lessons can be drawn from this study:
- The community video approach was effective even without follow-up home visits.
From its initial implementation in India in 2012, DG’s gold standard for community videos has always included follow-up home visits approximately two weeks following dissemination. Conducted by trained mediators, these follow-up visits are considered a crucial step in reinforcing key messages with the target population. In Burkina Faso and Niger, where SPRING piloted community videos, home visits were an integral part of the intervention package. Given how resource intensive household visits can be, one of our study objectives aimed to compare the effectiveness of the gold standard to a less expensive and more scalable approach that excludes these visits. While we were unable to conduct this analysis due to difficulties in properly scaling home visits, we consider the fact that disseminators were unsuccessful in conducting household visits among at least 50 percent of the target homes a telling finding. For projects that utilize volunteer mediators as is the case in Senegal, the time opportunity cost for conducting home visits may be too high to scale or sustain. Our experience in Senegal, however, demonstrates that participants learned and retained many key messages by attending a film screening and engaging in a facilitated group discussion, without the benefit of follow-up home visits. This simpler approach may provide a more practical option where time and budget constraints are significant. This finding also has implications for programs considering the use of community video more broadly and at a much larger scale. Using multiple communication channels to reiterate key messages supports desired behavior change.
For certain indicators, endline results showed improvements in control villages, which only received SPRING-supported nutrition- and hygiene-related radio broadcasts. Specifically, we saw statistically significant increases in the percentage of women who knew the benefits of colostrum, fed their child the minimum number of times, and fed their child from a separate plate, although these increases were not as large as those seen in the intervention group, where beneficiaries also viewed community videos on target themes. These findings suggest that radio is an excellent way to share information broadly and begin to catalyze change through targeted messages. The addition of community video, as a more direct communication channel, enhances results by reinforcing key messages heard elsewhere.
Additional evidence is needed to understand the lack of improvement in certain indicators, such as knowledge of critical moments for handwashing. Furthermore, studies one and two years post-intervention in other SPRING countries have shown some decline in desired nutrition and hygiene behaviors (Dougherty et al 2017). A similar follow-up in Senegal would provide further evidence on whether and why knowledge and practices decrease over time, and could provide insight on strategies to avoid this decline.
References
Agence Nationale de la Statistique et de la Démographie (ANSD) [Sénégal], et ICF. 2017. Sénégal : Enquête Démographique et de Santé Continue (EDS-Continue 2016). Rockville, Maryland, USA : ANSD et ICF.
Bandura, A. 2004. “Health Promotion by Social Cognitive Means.” Health Education & Behavior 31(2): 143-64. http://doi.org/10.1177/1090198104263660
Black, R. E., L. H. Allen, Z. A. Bhutta, et al. 2008. “Maternal and Child Undernutrition: Global and Regional Exposures and Health Consequences. ” Lancet, 371(9608): 243–60.
Dougherty, Leanne, Marjolein Moreaux, Chaibou Dadi, and Sophie Minault. 2017. Seeing Is Believing: Evidence from a Community Video Approach for Nutrition and Hygiene Behaviors. Endline Evaluation. Arlington, VA: Strengthening Partnerships, Results, and Innovations in Nutrition Globally (SPRING) project.
Stokols, D. 1996. “Translating Social Ecological Theory into Guidelines for Community Health Promotion.” American Journal of Health Promotion 10(4): 282-98.
World Bank. 2004. Le manuel de l'initiative de lavage des mains : guide de preparation d'un programme de promotion du lavage des mains au savon (French). Water and Sanitation Program. Washington, DC: World Bank.