In this slide document, we present findings from a fourth round of data collection completed in May 2017 in Niger to measure the sustained effect of the community video activities. The study focuses on handwashing and responsive feeding (feeding from a separate dish).
View the original Seeing is Believing report.
Niger’s Context
Niger, located in the Sahel region of West Africa, is characterized by harsh climate conditions that contribute to structural food crises and high rates of severe acute malnutrition among children. In 2012, the under-five mortality rate was 127 per 1,000 live births and 43.9 percent of children under five years of age were stunted (INS and ICF International 2012). A number of factors contribute to the high levels of child deaths and malnutrition, including childhood illness and inadequate dietary intake. Underlying determinants of malnutrition include household food insecurity, poor childcare practices, insufficient health services, and an unhealthy environment (Black et al. 2008). Many of these underlying determinants are influenced by cultural norms and practices, including polygamy, an emphasis on male decision-making, and low levels of literacy (Moreaux 2015).
Introduction
The World Health Organization (WHO) recommends a number of interventions to prevent diarrheal diseases, which contribute to nutritional deficiencies, reduced resistance to infections, and infants and young children (IYC) (Bentley, Wasser, and Creimpaired growth and development (WHO 2015). These interventions include handwashing with soap at critical times, for example, after toilet use. There is also an increasing recognition that feeding behaviors and styles can influence complementary feeding outcomes and dietary intake and thus the growth of ed-Kanashiro 2011). Promoting practices that support appropriate feeding behaviors and styles as well as hygiene requires highly contextualized social and behavior change communication (SBCC) strategies that address the constraints presented in rural, traditional, resource-constrained societies such as Niger.
SBCC is uniquely challenging in remote areas. It can be difficult to engage rural populations because of poor infrastructure and limited access to health care, both of which make it challenging for health workers to reach those most in need. Mass media approaches typically require access to radio or television, but in Niger, less than 50 percent of households in rural areas own a radio and only 3 percent in rural areas own a television (INS and ICF International 2012).
In addition, information often flows outward from urban centers, where a small group of people and interests determine which information rural communities should receive, rather than tailoring media content and allowing adaptation of information to the needs of rural communities based on an exchange of ideas and requests (Berrigan 1979).
The use of video as an SBCC medium offers several advantages when working in rural communities, such as more standardized content with fewer inconsistencies across educators, and high receptivity and understanding among low-literacy populations. Behavior change approaches that incorporate videos coupled with guided discussions at the community level have shown promise in public health (Desta et al. 2014; Khoury et al. 2002; Roye and Hudson, 2003; Tuong, Larsen, and Armstrong 2014). However, evidence is limited on the use of community videos to specifically support Maternal, Infant, and Young Child Nutrition (MIYCN) and hygiene behaviors.
Description of the Intervention
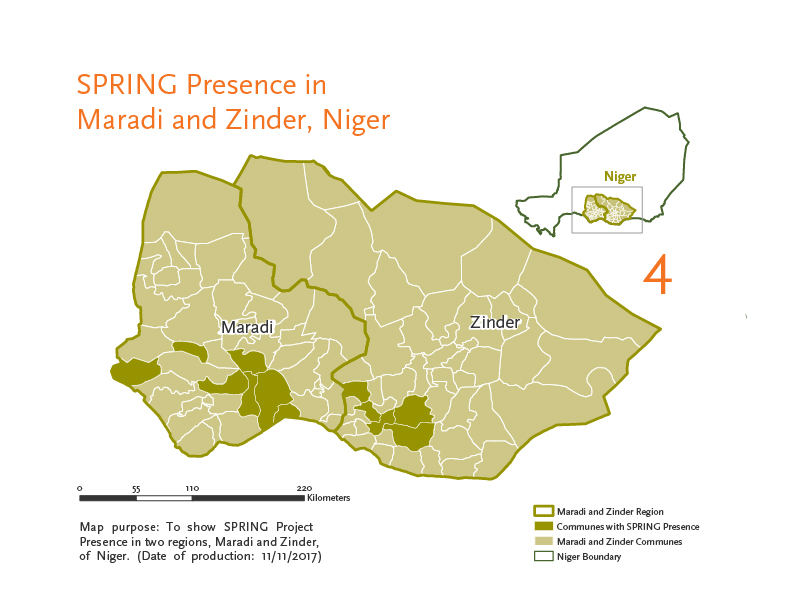
Between January and December 2015, the SPRING project implemented a community video approach in collaboration with Digital Green, REGIS-ER, Save the Children, and Mercy Corps with a total of 80 community groups in 20 villages in Niger’s Maradi region. Videos were screened among four community groups in each village, and were followed by facilitated discussions. A list of the implementation steps for the community video approach can be found in the figure to the left.
Following the successful pilot of the intervention, activities were scaled up to 115 villages in 2016 (61 villages in Zinder and 54 in Maradi). In 2017, the community video approach was expanded to 131 additional villages in these regions.
In 2015, SPRING conducted a mixed-methods evaluation to assess the feasibility, acceptability, effectiveness, sustainability, and costs associated with the community video approach. Findings are available here.
In this slide document, we present findings from a fourth round of data collection completed in May 2017 to measure the sustained effect of the community video activities. The study focuses on handwashing and responsive feeding (feeding from a separate dish).

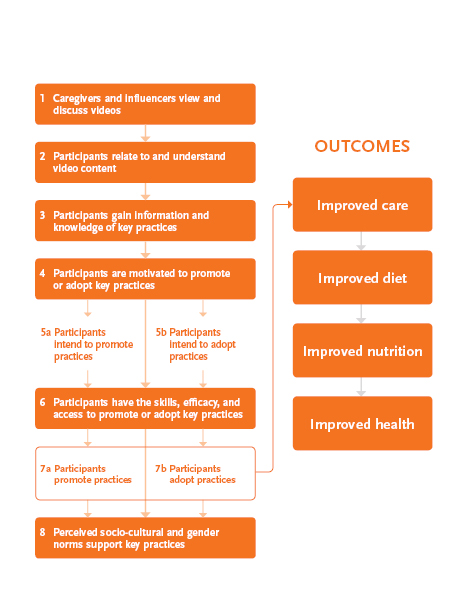
Conceptual Framework
The SPRING community video conceptual framework summarizes the pathways of change through which the intervention aims to improve handwashing and responsive feeding behaviors.
The intervention focuses on sharing information to improve knowledge about, and attitudes toward the behaviors of interest. The videos show actual community members practicing these behaviors, thereby demonstrating to viewers they can develop self-efficacy to practice the behaviors. Finally, by giving members of women’s groups the option to invite people who have an influence on their behaviors to video screenings, the intervention addresses social norms that are important determinants of behavior in the Niger context.

Study Objective
To measure the sustained effect of the community video approach on nutrition and hygiene behaviors.
Data
- Sample: Approximately 300 women exposed to the intervention who had children ages 6–23 months at the time of the intervention
- Study Design: Pre-post intervention household survey
- Setting: 20 villages in the Maradi region
- Study Period: Respondents interviewed in April 2015, June 2015, August 2015, and May 2017*
- Analysis: Bivariate analysis
*Results presented for the 1st, 3rd, and 4th data collection point in this document because the 2nd & 3rd data collection point were only two months apart.
Study Outcomes
The household surveys collected information on knowledge, attitudes, self-efficacy, and behaviors related to handwashing and responsive feeding. Indicators assessing behaviors were self-reported except where indicated below, and are explained in greater detail in the following slides.
Handwashing
- Indicator 1: Percentage of households with at least one place designated to wash hands (observed by interviewer)
- Indicator 2: Percentage of households with handwashing station with soap and water (observed by interviewer)
- Indicator 3: Percentage of handwashing stations maintained by the husband
- Indicator 4: Percentage of households with handwashing station near the latrine or kitchen (observed by interviewer)
Responsive Feeding
- Indicator 5: Percentage of women who fed their child with a separate plate at each meal
- Indicator 6: Percentage of women who actively encouraged their child to eat
- Indicator 7: Percentage of women who said their child was helped by responsible person at the last meal
- Indicator 8: Percentage of women who said that the person responsible for helping their child was less than an arm’s length away
Handwashing Messages
SPRING worked with local communities to produce a video on improving hygiene behaviors. Behaviors promoted in the video included—
- installing a handwashing station in the home, preferably near a latrine or the kitchen;
- ensuring that the handwashing station had soap and water available;
- encouraging proper handwashing techniques;
- encouraging husbands to maintain the handwashing station.
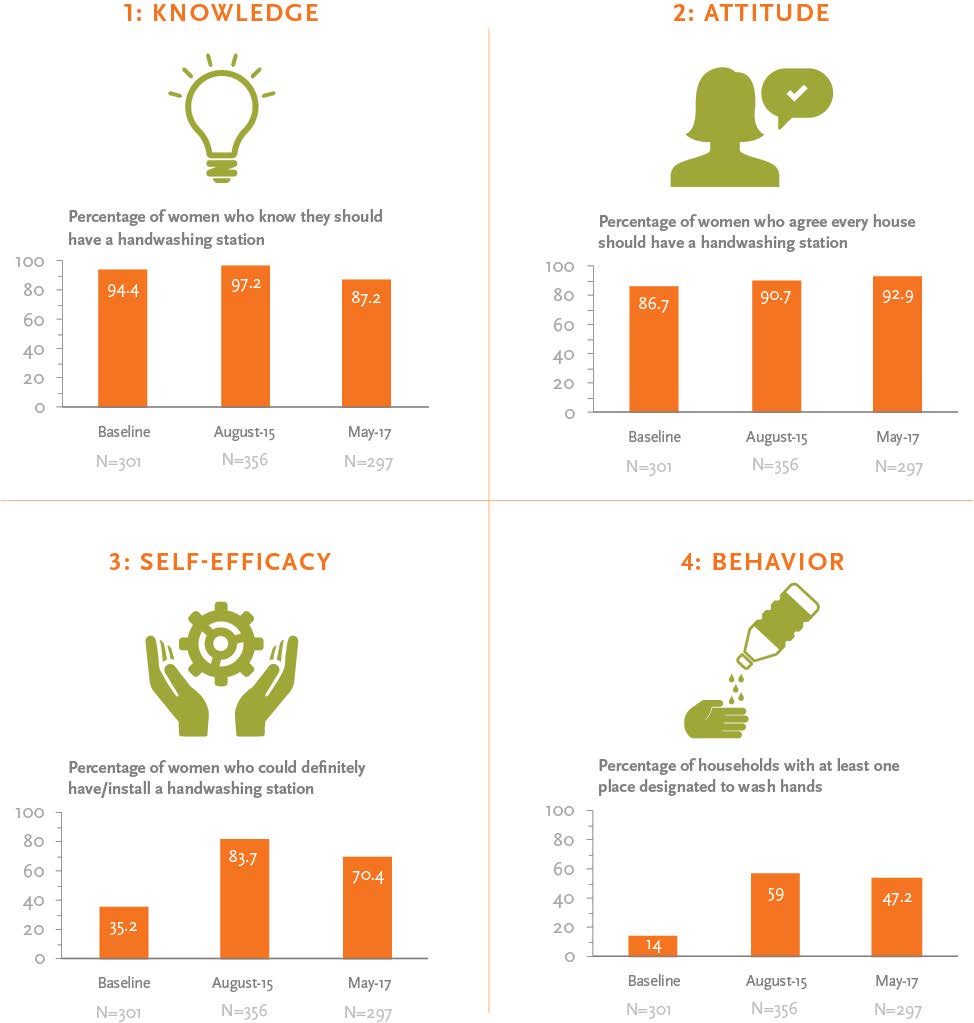
Indicator 1: Presence of a Handwashing Station
We asked women about their knowledge, attitudes, self-efficacy, and behaviors related to having a handwashing station. There was a decrease from the endline survey and follow-up survey in knowledge about the importance of having a handwashing station, yet a slight and sustained increase over time in the percentage of women who agreed that everyone should have a handwashing station. Women who said they could install a station increased and then declined two years after the intervention. A much higher percentage of households had handwashing stations after the intervention.
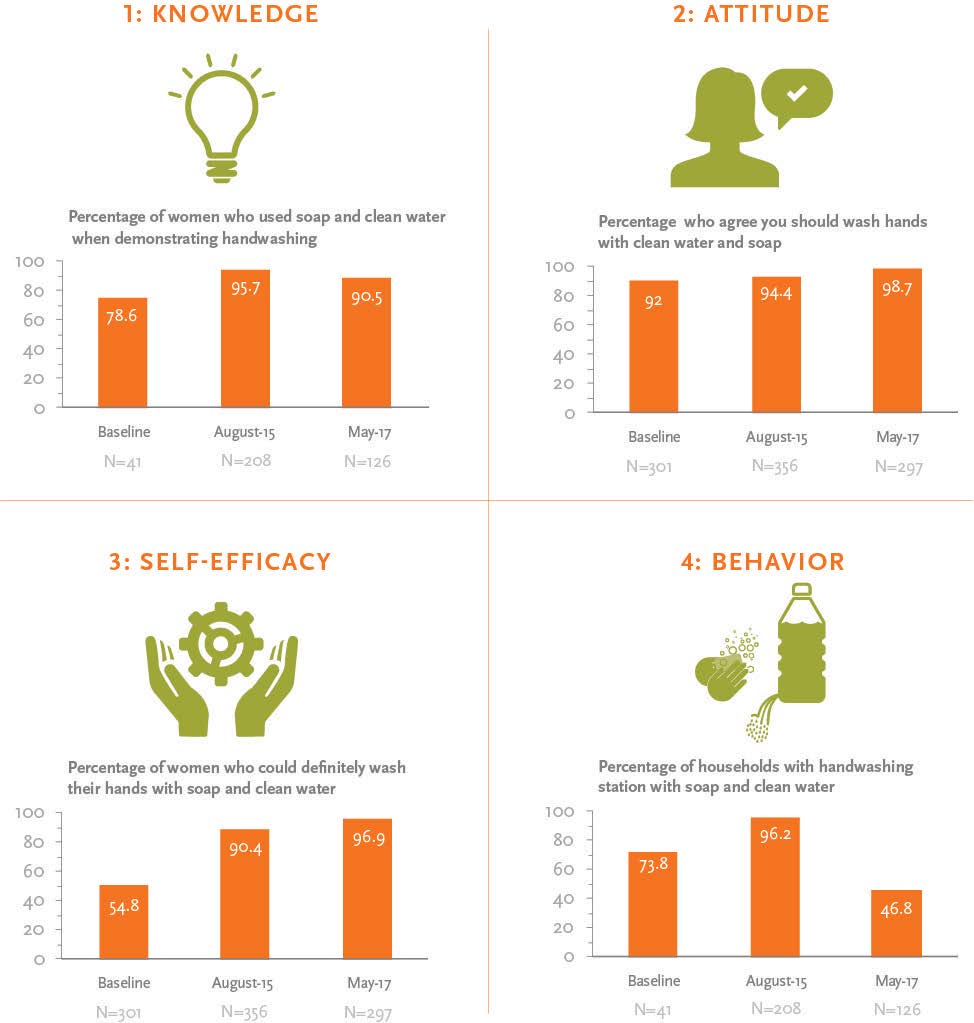
Indicator 2: Handwashing with Soap and Water
After the intervention ended, there was a slight decline in the percentage of women who demonstrated soap and clean water use while handwashing. However, we found a sustained increase over time in the percentage of women who agreed that everyone should wash with soap and clean water and who said they could use soap and water following the intervention. Despite these positive attitudes, we found that the percentage of women who had soap and clean water at a handwashing station was not sustained over time following the intervention.
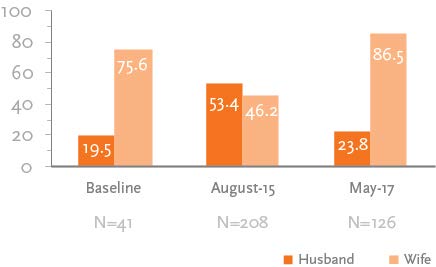
Indicator 3: Maintenance of Handwashing Stations
There was an increase in the percentage of husbands who were responsible for maintaining the handwashing station following exposure to the intervention in August 2015. However, this behavior was not sustained two years after exposure to the intervention. By May 2017, 86.5 percent of women reported that they were the primary person responsible for maintaining the handwashing station in the household.
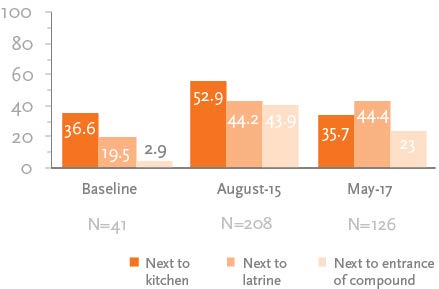
Indicator 4: Households with Handwashing Station Near the Latrine or Kitchen
The community video intervention promoted the placement of handwashing stations near kitchens and latrines and the results indicate that households adopted this practice, particularly near latrines. At baseline, 37 percent had a handwashing station near the kitchen, nearly 20 percent had such stations next to the latrine, and fewer than 5 percent had them next to the compound. After the intervention, we found increases in the number of handwashing stations across all locations. However, these increases declined two years following the intervention except for those next to latrines. Placement of handwashing stations near latrines increased from approximately 20 percent at baseline to 44 percent following the intervention and remained at the same level two years after the community videos were shared.
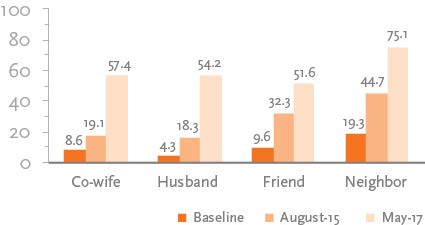
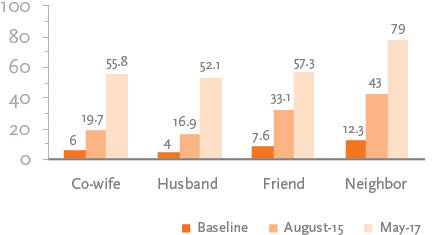
Percentage of Women who Shared Handwashing Message by Person Specified
The community video approach encouraged participants to promote information from the videos with others in the community. In this respect, we found that there were considerable and continued increases in sharing information about handwashing. At baseline, less than 10 percent of respondents shared information with co-wives, husbands, friends, and neighbors. Two months following exposure to the intervention, sharing messages with co-wives, husbands and neighbors had doubled, while sharing messages with friends had tripled. Two years after the intervention, we found that women were still sharing messages about handwashing with co-wives, husbands, and friends, ranging from roughly 50 percent among friends to 75 percent with neighbors.
Responsive Feeding Results
During the intervention period, SPRING worked with local communities to produce a video that focused on improving responsive feeding behaviors. Behaviors promoted in the video included—
- ensuring that the child has a separate plate for meals;
- encouraging responsive feeding techniques;
- having a responsible person within arm’s length of the child at meals;
- ensuring that a responsible person assists a child at meals.
Indicator 5: Child Has a Separate Plate
We asked women about their knowledge, attitudes, self-efficacy, and behaviors related to having a separate plate for their child. After the intervention was completed, we found a slight decline over time in knowledge and attitudes about the need for a child to have a separate plate. Despite these declines, we found an increased percentage of women who said they could provide their child a separate plate two years following the intervention. We also found that although the percentage of women who had a separate plate for their child declined two years after the intervention, it was still higher than prior to initiating the community video approach.
![a pair of hands with a gear in between them] Percent](/sites/default/files/publications/briefs/images/niger_slides_seeing_img10.jpg)
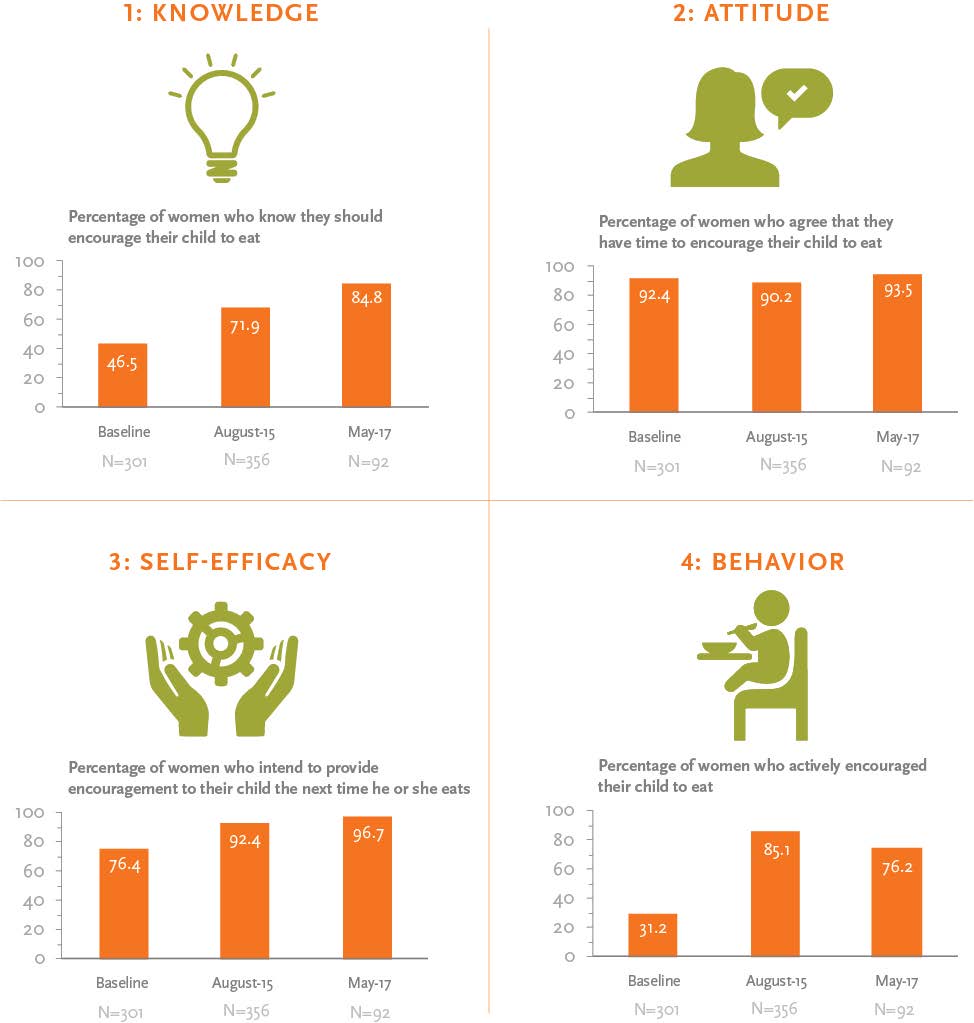
Indicator 6: Encouraging Child to Eat
After the intervention, caregivers greatly increased the practice of encouraging their child to eat. Two years later, there was a continued increase in knowledge, attitudes, and self-efficacy related to providing encouragement to the child to eat, but a decline in the percentage of women who actually carried out the practice. Despite this decline, this measure of responsive feeding* was still higher than at baseline.
*Responsive feeding was calculated based on a battery of 20 validated questions that have been shown to measure if a caregiver is actively feeding the child.
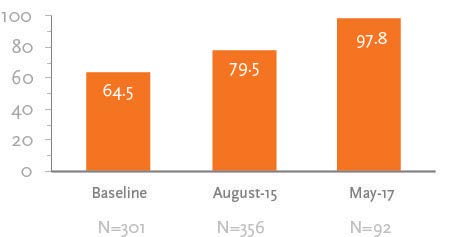
Indicator 7: Responsible Person was Less than an Arm’s Length Away from Child
Among women who had a child between 6-23 months of age during the intervention and who currently have a child in this age category, we asked if they had a responsible person less than an arm’s length away at their child’s last meal. We found that at baseline, approximately two-thirds of women said a responsible person was an arm’s length away from their child at the last meal. This increased to nearly 80 percent two months following the intervention and to approximately 98 percent two years following the intervention.
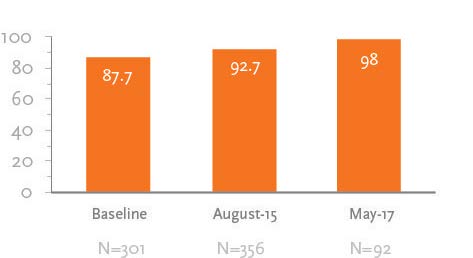
Indicator 8: Child was Helped by a Responsible Person at Their Last Meal
Among women who had a child between 6-23 months of age during the intervention and who currently have a child in this age category, we asked if their child was helped by a responsible person at their last meal. We found that at baseline, approximately 88 percent of women said a responsible person helped their child at their last meal. This increased to nearly 93 percent two months following the intervention and to 98 percent two years following the intervention.
Sharing Information on Responsive Feeding
The community video approach encouraged participants to promote information from the videos with others in the community. We found that there was considerable and continued increases in sharing of information related to responsive feeding. Among women who were exposed to the community videos, we found that at baseline, less than 15 percent had held conversations on responsive feeding with co-wives, husbands, friends, and neighbors. Two months following the intervention, information sharing increased significantly; these increases were even more significant two years after the intervention.
Conclusion
- The community video approach proved effective in improving and sustaining knowledge, attitudes, self-efficacy, and self-reported behaviors in Niger.
- While feeding and hygiene behaviors improved following the intervention and remained higher than at baseline two years later, there were some declines over the two-year period.
- Inviting influential individuals, especially husbands, to carry out or support intervention activities increases their immediate engagement but does not translate into sustained support.
Recommendations
- There is a need for periodic or “refresher” video viewings to maintain some of the behavior change that occurred immediately following exposure to the community video approach.
- There is a need to test new approaches to engage and maintain male involvement in behavior change, such as involving community leaders to encourage men to adopt more supportive family behaviors.
- Evidence is needed to understand how messages shared with friends and neighbors translate into behavior change among populations who were not directly exposed to the community video approach.
View the full report, Seeing is Believing, here.
References
Bentley, M. E., H. M. Wasser, and H. M. Creed-Kanashiro. 2011. “Responsive Feeding and Child Undernutrition in Low- and Middle-Income Countries. ” Journal of Nutrition 141(3): 502–507. http://doi.org/10.3945/jn.110.130005
Berrigan, F. 1979. Role of Community Media in Development. Paris: United Nations Educational, Scientific and Cultural Organization.
Black, R. E., L. H. Allen, Z. A. Bhutta, et al. 2008. “Maternal and Child Undernutrition: Global and Regional Exposures and Health Consequences. ” Lancet, 371(9608): 243–60.
Desta, B. F., H. Mohammed, D. Barry, A. H. Frew, et al. 2014. “Use of Mobile Video Show for Community Behavior Change on Maternal and Newborn Health in Rural Ethiopia.” Journal of Midwifery & Women’s Health 59(s1): S65–S72. http://doi.org/10.1111/jmwh.12111
Institut National de la Statistique (INS)and ICF International. 2012. Enquête Démographique et de Santé et à Indicateurs Multiples du Niger 2012 [French]. [Multiple Indicator Demographic and Health Survey.] Calverton, MD: INS/ICF International.
Khoury, A. J., A. K. Mitra, A. Hinton, et al. 2002. “An Innovative Video Succeeds in Addressing Barriers to Breastfeeding among Low-Income Women.” Journal of Human Lactation 18(2): 125–31.
Moreaux, M. 2015. Informing Video Topics and Content on MIYCN and Handwashing: Situational Analysis and Formative Research in Maradi, Niger. Arlington, VA: Strengthening Partnerships, Results, and Innovations in Nutrition Globally (SPRING) project.
Roye, C., and M. Hudson. 2003. “Developing a Culturally Appropriate Video to Promote Dual-Method Use by Urban Teens: Rationale and Methodology.” AIDS Education and Prevention 15(2): 148–58.
Tuong, W., E.R. Larsen, and A. W. Armstrong. 2014. “Videos to Influence: A Systematic Review of Effectiveness of Video-Based Education in Modifying Health Behaviors.” Journal of Behavioral Medicine 37(2): 218–33. http://doi.org/10.1007/s10865-012-9480-7

