
Executive Summary
The SPRING project began work in Ghana in 2014 in response to a request from USAID/Ghana for support to reduce stunting in the Feed the Future zone of influence in the Northern and Upper East Regions of the country. To help achieve this goal and improve nutrition in these areas, SPRING developed the “1,000-day household approach.” This was a multi-sectoral strategy focused on linking nutrition, water, sanitation, and hygiene (WASH), and agriculture with an emphasis on priority household actions to address the underlying causes of poor nutrition among pregnant women and children under 2 years of age. The first 1,000 days is a critical time to intervene to prevent stunting in young children because it is a time of rapid growth and development. Failure to ensure adequate nutrition during the first 1,000 days can lead to lifelong stunting, a diminished capacity to learn, poor performance in school, and increased susceptibility to infection and disease.
Given that behavior change occurs through multiple channels and levels, SPRING worked at both the community and facility levels to improve nutrition. With our infant and young child feeding (IYCF) work, we helped to significantly improve the quality of IYCF services at health facilities by revising and providing updated counseling materials and providing training to health providers on correctly monitoring child growth over time to provide targeted counseling to caregivers and mothers. We trained and supported over 1,500 facility-based health providers and 2,400 community health volunteers who conducted peer education and behavior change support in 1000-day households within their respective communities. SPRING also piloted a father-to-father support group program to engage more men, especially fathers, on issues of malnutrition prevention and IYCF promotion. SPRING’s investment in IYCF and other nutrition activities was successful; we saw stunting reduce from 20.9 percent to 16.9 percent among children under two in SPRING-supported areas.
To ensure quality provision of health services at both the facility and community levels, we established a quality improvement (QI) program to examine how nutrition service delivery could be improved to help staff provide better care and to increase demand for nutrition services from the community. We ultimately trained staff at 95 health facilities and 150 community teams in this approach who are still active in the communities where we worked.
Because anemia has remained a challenging health issue for women and children in 1,000-day households, we designed and rolled out a comprehensive multi-sectoral anemia reduction program package which we used to train over 450 staff from across 280 health facilities in our zone of influence. From this, we saw immediate results in rapid increases in hemoglobin testing and improvement in the quality of anemia counseling for pregnant women attending antenatal care services. We also successfully introduced and piloted the use of a district assessment tool for anemia which allowed local districts to better collect information about the underlying causes of anemia in their areas and help them to use data to address these causes.
Our WASH approach was also designed around the 1,000-day household. We referred to activities under this heading as “WASH 1,000” included community-led total sanitation plus a focus on four key hygiene behaviors: disposal of child and adult feces, handwashing at critical times, the promotion of clean drinking water, and the creation of clean play spaces for children. At the end of our project, over 9,000 households had built latrines in the 405 communities where we worked. A total of 193 communities were also declared open defecation free.
We based our agriculture approach on the farmer field school model and focused on aflatoxin reduction in groundnuts to increase the safety of this nutrient-rich staple food. As a result of our work on aflatoxin prevention and reduction, we increased the prevalence of farmer knowledge about aflatoxin from 22.1 to 49.2 percent. Our agriculture work also included promoting consumption of nutrient-dense foods, including orange-fleshed sweet potatoes and vitamin A-enriched maize.
To promote and support adoption of nutrition-related behaviors, nearly all of SPRING’s activities included a social and behavior change communication component, reinforcing key messages at each point of contact with beneficiaries, from health service to formation of mothers groups and farmer field schools. These activities were guided by the use of media such as videos shown at community events, radio, and short instructional videos and photo aids, in addition to broad nutrition communications and advocacy.
To help ensure the sustainability of our work, SPRING collaborated closely with existing government and nongovernmental organizations. To achieve this, we engaged partners at multiple levels, particularly at the district and regional levels. We also invested in building and expanding the technical capacity of government sector departments and community organizations supporting nutrition-specific and nutrition-sensitive interventions. This approach helps ensure the existence of institutional capacity to enable future scale-up of activities beyond the life of SPRING.
SPRING in Ghana
Background
In northern Ghana, 33 percent of children under the age of 5 years are stunted compared with only 10 percent in the greater Accra region.1 According to the most recent Demographic and Health Survey, the Northern region of the country continues to have the highest rates of malnutrition with 20 percent of children under the age of 5 years measuring as underweight. While nationally rates of stunting have gone down since 2008, rates in the Northern region have increased from 32 to 33 percent. Rates of exclusive breastfeeding also remain low. Overall, 56 percent of women reported initiating breastfeeding within one hour of birth, and the percent of children who were exclusively breastfed to the age of six months was only 52 percent.
The Northern region has historically received less attention from various stakeholders, in part because of the lower population density. However, this has begun to change in recent years, with more nongovernmental organizations (NGOs), donors, and implementing partners increasing their support for government health and agriculture efforts in the region. The United States Agency for International Development (USAID) has expanded investment efforts in northern Ghana over the past few years, with Feed the Future initiatives and several health projects in many sectors, including behavior change communication; water, sanitation and hygiene (WASH); governance and development; and health systems strengthening.
To reduce rates of malnutrition and stunting in children, there is a need for earlier interventions in households within the critical period of the first 1,000 days—from pregnancy to a child’s second birthday. This is a developmental window where the greatest impact can be made on prevention of malnutrition. By recognizing and leveraging the opportunity to teach 1,000-day households (households with pregnant or lactating women and children under 2 years of age) about vital health and nutrition messages, great progress can be achieved in reducing rates of malnutrition.
SPRING Goals and Objectives
SPRING began work in Ghana in 2014 after receiving a concept note from USAID/Ghana requesting support to reduce stunting by 20 percent in the Feed the Future zone of influence (ZOI) in the Northern and Upper East Regions of the country. The concept note proposed delivery of a broad range of evidence-based nutrition interventions to reduce stunting in up to 15 districts chosen for their relatively high rates of stunting. To help achieve this goal, the project focused on these five objectives:
- Objective 1: Improved delivery of high-impact nutrition services;
- Objective 2: Increased demand for high-impact nutrition practices and services;
- Objective 3: An improved enabling environment for adoption and delivery of high-impact nutrition practices and services;
- Objective 4: An enhanced evidence base regarding delivery of selected high-impact interventions;
- Objective 5: An enhanced policy environment for delivery of state-of-the-art nutrition interventions.
SPRING Approach
The 1,000-Day Household Approach
To achieve our five main objectives, we developed a framework for our technical assistance referred to as the “1,000-day household approach.” Under this strategy, we focused on key nutrition-specific and nutrition-sensitive household behaviors targeting the underlying causes of malnutrition (see figure 1). We began by choosing 10 communities within a district each program year, prioritizing key behaviors within households that had a pregnant woman or a nursing mother with a child under 2 years old.
We rolled out our programs by building the technical capacity of various Government of Ghana sector staff, including the District Health Management Teams, Environmental Health and Sanitation Unit, the District Agriculture Development Unit, the Education Service, and the Community Development and Social Welfare Department. The trained technical personnel then formed or mobilized community-level volunteer networks in health, agriculture, and WASH, and collaborated with local NGOs and civil society organizations with established credibility and experience to support the 1,000-day household-level behavior change activities.
Figure 1. A Framework of the Integrated 1,000-Day Household Approach and Key Behaviors
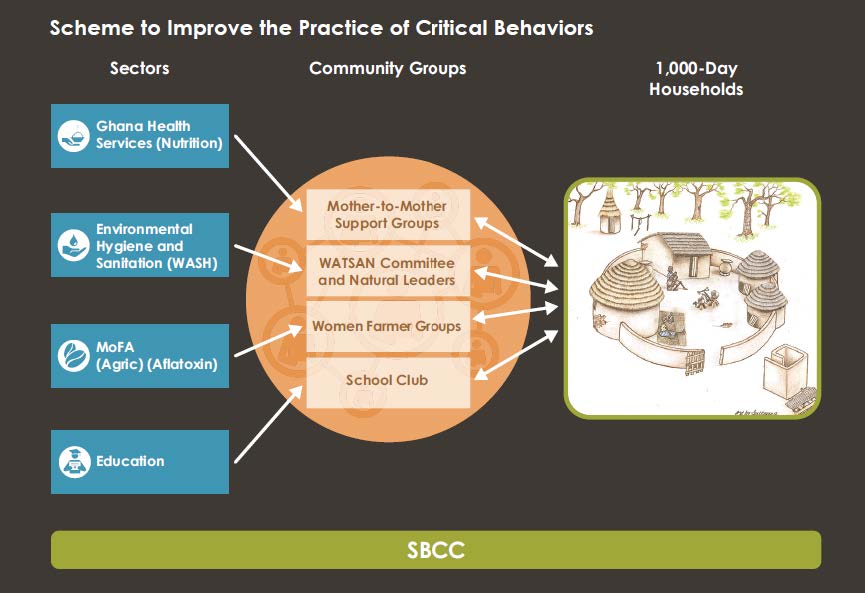
Figure 2. Map of SPRING Operational Districts

Interventions and Coverage
Between 2014 and 2017, SPRING covered 15 districts in the Upper East and Northern regions of Ghana (see figure 2). In FY 2015, we worked in 10 communities per district, and added an additional 10 communities in FY 2016. In our final year, we targeted seven communities per district, bringing the total number of communities we worked in over the life of the project to 405. SPRING partnered with the governing assemblies in each district to select the communities at the beginning of each program year. This was done after holding national level consultations and conducting regional inception meetings.
Based on the regional-level experience, we realized it was critical to explore the district context to formulate program plans that respond to district staff and available personnel’s capacities and experiences. We conducted scoping visits to all 15 districts to map existing and ongoing nutrition-specific and nutrition-sensitive interventions. This helped us to formulate our workplans and activities. By working closely with the government and other local partners, SPRING was ultimately able to train over 45,000 people on nutrition-sensitive and specific topics. We helped 137 communities become certified as open defecation free, widely increased knowledge of aflatoxin, and helped to reduce stunting within our ZOI.
Major Accomplishments
Over the life of the project, SPRING made significant progress in reducing malnutrition within our ZOI. Information obtained from our baseline (2015) and endline (2017) surveys (see table 1) shows that SPRING activities were able to reduce stunting from 20.9. percent to 16.9 percent among children under 2 years of age. This positive change was also reflected in improved nutrition behaviors as indicated by increases in the prevalence of exclusive breastfeeding for children under 6 months (from 84.3 percent to 87.3 percent) and appropriate introduction of complementary feeding (from 52.4 percent to 64.1 percent). Prevalence of children under two receiving the minimum acceptable diet increased more than threefold, from 9.5 percent to 29.5 percent. Other household behaviors showed further improvements, including: an increase in the percentage of households reached with social and behavior change communication (SBCC) activities (from 66.6 percent to 95.5 percent); an increase in the number of people who could correctly mention three critical times of handwashing (from 51.9 percent to 64.1 percent); a more than tenfold increase in the percentage of households with tippy taps at the recommended places (from 1.4 percent to 16.6 percent); and an increase in the percentage of households with groundnut storage systems that meet criteria for aflatoxin reduction (from 10.3 percent to 25.4 percent).
Table 1. SPRING Household Baseline to Endline Assessment Comparison
| Indicator | Baseline (2015) % | Endline (2017) % |
|---|---|---|
| Prevalence of stunted children under 2 years of age | 20.9 | 16.9 |
| Prevalence of exclusive breastfeeding of children under 6 months of age | 56.8 | 87.2 |
| Appropriate introduction of complementary feeding among children 6–8 months | 52.4 | 64.1 |
| Prevalence of children age 6–23 months receiving a minimum acceptable diet | 9.5 | 29.5 |
| Percentage of households reached by SBCC activities | 66.6 | 95.5 |
| Percentage of households with functional tippy taps in recommended locations | 1.4 | 16.6 |
| Percentage of household respondents who know any three critical times of handwashing | 51.9 | 64.1 |
| Percentage of farmers with accurate knowledge of aflatoxin levels | 22.1 | 49.2 |
| Percentage of households with groundnut storage systems meeting criteria for reducing aflatoxin levels | 10.3 | 25.4 |
Infant and Young Child Feeding (IYCF)
When SPRING first started work in Ghana, Ghana Health Service (GHS) was implementing a variety of programs for improving nutrition services to help increase awareness about malnutrition, promote early initiation and exclusive breastfeeding, and improve knowledge about introducing complementary foods. Despite these and other efforts, major gaps existed with service performance, which GHS attributed to inadequate numbers of trained staff, poor quality of the training activities, shortages of logistics and supplies, lack of monitoring and supervision, poor availability of transport, and lack of volunteer support for community engagement in nutrition. SPRING analyzed the situation and found that, to improve service delivery and have a greater impact on nutrition, we should focus on improving the quality of IYCF counseling and services at both the health facility and community levels.
IYCF at the Health Facility Level
To improve IYCF services at the health facility level, SPRING trained 1,528 health staff from over 280 health facilities within our ZOI. These trainings focused on correctly monitoring child growth over time, with a particular emphasis on accurately filling out growth charts to help identify trends and provide targeted counseling to caregivers and mothers. Through information gathered from supervision visits to health facilities conducted by the GHS and SPRING staff, we found that, prior to our intervention, the number of child growth records correctly and completely filled was very low. Over the life of our project, regular supervision visits showed a steady improvement in this number, which averaged between 60 and 80 percent at the project’s end. SPRING also helped to revise the IYCF supervision checklist at the regional level, emphasizing the importance of correct growth charting, triaging, targeted counseling, and on-the-job demonstrative trainings to strengthen service providers’ IYCF skills.

IYCF at the Community Level
At the community level, SPRING worked to improve IYCF practices by leveraging community volunteers to support health care service delivery at outreaches (satellite service points in communities) and to conduct health promotion activities locally. Working with the existing UNICEF community IYCF (C-IYCF) training manuals, SPRING created a training curriculum aimed specifically at community health volunteers (CHVs). Using this guide, SPRING trained 2,477 CHVs. This ensured the availability of one or two CHVs for each of our 405 communities, and created a group of trained CHVs to serve other communities after SPRING. These trained CHVs provided support to health workers in IYCF service delivery both at the health facilities and during outreach visits conducted in their respective communities. The CHVs also served as facilitators of community groups—for example, mother-to-mother support groups (MTMSGs)—held monthly meetings, and conducted peer education on IYCF at the household level.
Mother-to-mother support groups provide important community platforms for health and nutrition information sharing as well as a way to motivate positive behavior change. Following a similar process as with the C-IYCF guide for CHVs, we drafted a training curriculum for MTMSGs and trained 4,843 women who participated in groups for 300 of our target communities. These groups met monthly to discuss different IYCF topics, including breastfeeding, complementary feeding, and hygiene practices that can have a positive impact on child health outcomes. These monthly discussions, facilitated by CHVs, included resources like the SPRING-developed facilitator’s guide, the UNICEF IYCF counseling cards, and a SPRING-developed radio serial program on IYCF topics. Group members were also encouraged to offer their own ideas and to support one another as caregivers.
Recognizing the importance of involving men in nutrition, SPRING also piloted father-to-father support groups (FTFSGs) in four communities in two of our districts. This innovative, gender-sensitive approach encouraged male community members to be influential change agents who positively contribute to good nutrition outcomes for their family members during the first 1,000 days. To train these groups, SPRING developed a FTFSG facilitator’s guide and accompanying counseling cards, adapted from the Infant and Young Child Feeding Project and the Infant and Young Child Nutrition men’s group package. The monthly group meetings focused on gender roles and effective communication and also on good IYCF and hygiene practices. At the end of each meeting, the men developed and implemented action plans for attaining improved child health and nutrition outcomes in their communities.
Quality Improvement (QI)
Through our work in both health facilities and in communities, we recognized the need to improve the processes and systems delivering nutrition services and to increase demand for quality nutrition-related services. Prolonged facility wait times and inaccurate monitoring of child growth were leading to frustration in communities and preventing appropriate care and counseling. To address these weaknesses, we decided to implement a two-pronged quality improvement (QI) program to look into how nutrition service delivery could be changed to help staff provide better health care and leverage existing systems to increase demand for nutrition services in the community. The QI approach is a well-known and widely used process for problem solving comprised of four steps—plan, do, study, and act (PDSA). In Ghana, we followed a facility- and community-owned problem solving process to identify gaps, and fill those gaps using low-cost, locally feasible solutions.
We began by conducting sensitization of the GHS regional and district directorates who helped us to identify seven districts with an interest in implementing this approach. We then trained 171 coaches and 481 facility-based health staff, who made up the QI teams for 95 health facilities. Theses QI teams met on a monthly basis and participated in exercises using the PDSA methodology—a process of identifying a problem, reviewing routinely reported data, analyzing and understanding the reasons for poor outputs, planning and scheduling change ideas, implementing actions, studying the results, and planning new actions. The trained coaches visited the QI teams monthly and assisted them through these steps.
On a quarterly basis, all of the QI teams in a district met to share their progress and experiences at learning session events. One of the districts, Kumbungu, reached a full year’s cycle of implementation and held a harvest session to showcase some of the highly successful change ideas they implemented with good results, such as:
- conducting random audits of child health record books to facilitate accurate filling of growth charts;
- conducting regular health education sessions to increase postnatal attendance;
- engaging CHVs to boost coverage in antenatal care clinic (ANC) attendance;
- increasing the number of ANC counseling sessions and improving record-keeping to enhance coverage and quality of ANC services;
- sensitizing communities on child immunization to increase coverage;
- visiting homes to increase the numbers of women achieving four or more ANC visits.
We also conducted QI at the community level within our selected districts to empower community members to take an active role in analyzing health or nutrition gaps and to demand quality services while also adopting positive health-seeking behaviors. Following the successful implementation of QI at local health facilities, we formed a total of 150 community QI (C-QI) teams, partnering with four local NGOs to provide support. These partner NGOs trained 176 C-QI coaches, most of whom were CHVs or community health nurses linked to the community. C-QI teams identified a number of successful change ideas and found that engaging families within their households was effective in encouraging positive behavior change, such as attendance at child welfare clinics (CWCs). For example, in one community, the C-QI team identified the root cause for low CWC attendance to be the long distance to get to the clinic. The team’s change idea involved sensitizing fathers to help ensure transport to the clinic for their wives and children. Through this, the monthly CWC attendance rate for children in the community increased from 52 percent to 100 percent in only four months.
Strengthening the Supply Chain
SPRING worked with the USAID | DELIVER project and GHS to conduct a situational assessment of the nutrition commodities supply chain in the Northern and Upper East regions. Findings from the assessment showed frequent stockouts of nutritional commodities, inadequate supervision, poor recordkeeping, and lack of transport. Collaborating with DELIVER, we organized refresher trainings for trainers at the regional level, leading to subsequent rollout of logistics management and information systems (LMIS) trainings for nutrition commodity managers and health staff and training 939 people in our 15 districts. These trainings were followed by quarterly monitoring visits. The LMIS capacity built showed evidence of increased use of commodity tally/control cards, improved commodity storage space, and decreases in stockout rates of some commodities across health facilities in our ZOI. We also supported the supply chain systems with targeted procurements contributed by SPRING to ensure the availability of essential commodities necessary for service provision (see table 2).
Table 2. Nutrition Commodities and Equipment Procured for SPRING Districts
| Item | Packing | Total Units Ordered | |
|---|---|---|---|
| 1. MUAC tapes (child) | 828 | tapes/polybag/carton | 8,726 |
| 2. MUAC tapes (adult) | 828 | tapes/polybag/carton | 8,726 |
| 3. Height Board | 6 | unit/carton | 264 |
| 4. Tarred weighing scales, Seca | 1 | unit/carton | 215 |
| 5. Baby scales, Seca | 1 | unit/carton | 215 |
| 6. HemoCue Hb 301 devices (Hb301) | 1 | unit/carton | 430 |
| 7. HemoCue Microcuvettes | 4 | unit/carton | 289,200 |
| 8. AA batteries for HemoCue Hb 301 and baby scales | 180 | unit/carton | 3,010 |
| 9. Ferrous sulphate 200 mg/folic acid 0.4 mg s/c | 50 | tabs/bottle/carton | 817,000 |
| 10. Vitamin A (retinol palmitate) 100,000 I.U. | 7 | caps/bottle/carton | 3,200 |
| 11. Water purification tablets | 1600 | strip of 10 tabs/carton | 1,402,086 |
| 12. ZinCfant 20 mg | 72 | blister of 10 tabs/carton | 56,830 |

Anemia
Anemia has remained one of the most challenging indicators in health status for women and children in 1,000-day households in Ghana, affecting 66 percent of children under five and 42 percent of women of reproductive age.2 To address this, our major project objectives included:
- understanding the current situation and burden of anemia in Ghana to inform a multi-sectoral program approach to address the anemia burden;
- developing a comprehensive curriculum for implementing an effective anemia control program involving both the health services and communities;
- instituting a multi-sectoral appraisal and response methodology using the District Assessment Tool for Anemia (DATA) to enable effective partners collaboration and coordination in anemia control activities at the district level; and
- supporting the strengthening of the national anemia policy and its dissemination to lower levels.

Anemia Training and Supportive Supervision
Using findings from an anemia landscape analysis we conducted in 2016, SPRING worked with the GHS Micronutrient Task Team to create a comprehensive anemia training curriculum for building the capacity of health workers and community health volunteers. A total of 459 health staff were ultimately trained on the determinants of anemia and current strategies and guidelines for treatment, especially in vulnerable groups, such as pregnant women and children under age five. These trainings also enabled the health workers to improve or acquire critical skills for nutrition counseling on anemia prevention/reduction, clinical examination to identify anemia, hemoglobin (Hb) testing using the HemoCue device, iron-folic acid supplementation and treatment regimes, and prevention of major infections, such as malaria, that contribute to anemia prevalence. Some of the trained health workers also received additional training skills, and subsequently went on to train and support 291 CHVs. These CHVs were then able to support MTMSGs in their respective communities to promote anemia prevention, just as they were doing with IYCF.
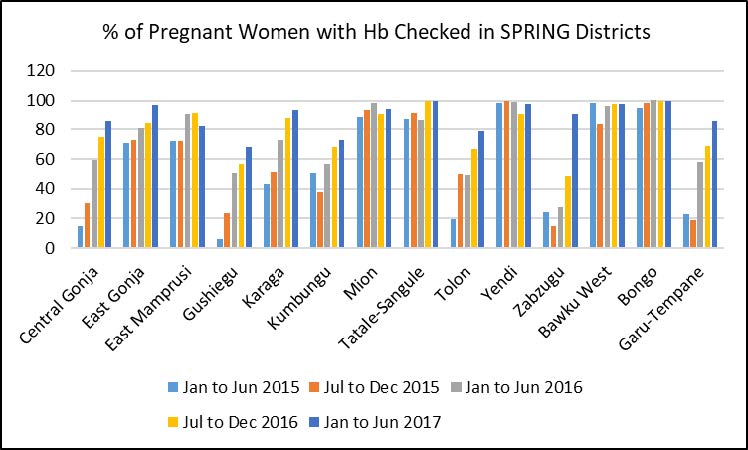
As a result of this improved capacity, there is now almost universal availability of Hb screening across all the health facilities within our ZOI, including at the primary care level (see figure 3). We also used an existing platform for sustained anemia prevention messaging and behavior change at the community level. With trained CHVs using an anemia discussion guide as part of the IYCF and maternal nutrition promotion topics, the MTMSGs included anemia topics to discuss during their monthly meetings.
Figure 3. Percentage of Pregnant Women with Hemoglobin Checked at SPRING Districts
District Assessment Tool for Anemia (DATA)
With support from home office technical experts, SPRING introduced the DATA tool to increase awareness about the multifaceted nature of anemia, better understand what drives anemia in a given context, and help districts plan and prioritize actions using local data to address immediate and underlying causes of anemia. SPRING first piloted DATA in Kumbungu District in 2015, working with the GHS Regional Health Directorate and the Kumbungu District Assembly. The pilot project brought together government staff from the health, water, agriculture, and education sectors to discuss the causes of anemia, analyze data, and prioritize anemia actions. This pilot project showed that DATA increased awareness of anemia as a problem that extends beyond the health sector and requires a multi-sectoral response. As one outcome of this awareness, the Ghana Education Service and GHS decided to synchronize their visits to schools under the school-based deworming program, instead of the previous approach of separate visits by each sector. In addition, the action plan devised by the agriculture sector involved changes to the training module for farmers on irrigation, to include measures to prevent standing water, a major environmental factor contributing to malaria and anemia.
Results of DATA field testing in Ghana in 2015 (along with Nepal and Uganda in 2016) led to SPRING streamlining the tool, adding indicator definitions, and refining the dashboards. Further, experiences and perspectives of country stakeholders during the field testing facilitated the development of our accompanying materials—user, facilitator, and training of trainers guides and PowerPoint presentations— for DATA implementation through facilitated workshops. The final version of DATA can be used globally, but customized to country context.
Spreading Good Ideas to Friends and Neighbors
In one small village in the Talensi District (Kpatia-Tengre) a lack of latrines resulted in community members openly defecating around homes and in fields. But when members of the community joined members of the nearby SPRING-supported Tualabare village to watch a video warning against the health risks that come from open defecation and poor sanitation, a few community members began constructing latrines with accompanying tippy taps around their homes. This led to a revolution in the Kpatia-Tengre community, with all the other households constructing their own latrines.
“After watching the community drama, we realized that the sanitation of our community had a lot to do with the cases of diarrhea [and] invasion of flies… We felt that there was a need to do something about it.” -Tengdo Kuzoba, resident of Kpatia-Tengre community
SPRING-trained government staff members were impressed by the community’s motivation and began providing guidance on how to improve sanitation across the whole community, through open defecation free (ODF) verification and certification. In a few months, the community participated in its first verification, which it failed due to incomplete latrines in two households. The community mobilized and supported those households to finish their latrines, and invited the verification team to return. This time, they passed and were declared ODF.
Water, Sanitation, and Hygiene (WASH)
SPRING’s WASH strategy in Ghana focused on enhancing the existing government strategy of community-led total sanitation (CLTS). The CLTS process aims to trigger communities to recognize the health risks of open defecation, which is practiced widely in Ghana, and to commit their own time and resources to constructing latrines and tippy taps (handwashing stations). SPRING brought our focus on households with pregnant and lactating women and children under 2 years of age to this strategy, creating a CLTS approach called WASH 1,000. This approach promotes constructing latrines and tippy taps, as well as emphasizing the health and nutritional benefits of good WASH practices. We focused on four key WASH behaviors for 1,000-day households:
- handwashing with soap or ash at critical times;
- safe disposal of human and animal feces;
- creating clean play spaces for children, free of contamination; and
- boiling water to make it safe to drink for children older than 6 months.
Before rolling out CLTS/WASH 1,000 in communities, we held training workshops for 618 environmental health officers (EHOs) and community development officers (CDOs). The officers were trained to effectively incorporate the nutrition and health components of WASH 1,000 in their communities served.
The CLTS approach occurs in three phases: pre-triggering, triggering, and post-triggering. During pre-triggering, EHOs and CDOs selected and entered communities in the 15 districts where we worked. They established relationships with the community and prepared them for the rest of the CLTS process. In the triggering phase, community members participated in a variety of exercises led by the EHOs and CDOs to sensitive them to the dangers of open defecation. Community members discussed their reasons for defecating in the open, mapped unclean areas of the community, and calculated both the amount of feces present in their community and the potential medical expenses associated with open defecation. After communities recognize the risks of open defecation and the need to change their behaviors, they enter the post-triggering phase, where they create plans for how to attain open defecation free (ODF) status.
To further show the need for improved WASH behaviors, we created a WASH 1,000 video with a local community drama group. The video emphasizes the four key WASH behaviors and shows some possible health consequences of poor WASH practices. It was screened in 366 of our communities, and has since been adopted as a standard step in the triggering phase of CLTS.
To help communities monitor their plans, we identified active community leaders who could keep the plan on track. We called these individuals natural leaders, and the groups were water and sanitation management teams (WSMTs). The natural leaders and WSMTs helped facilitate demonstrations by the EHOs and CDOs, checked in with neighbors about latrine construction, and kept their communities on track with their sanitation plans. During the life of the project, we trained 3,072 natural leaders and 2,168 WSMT members.

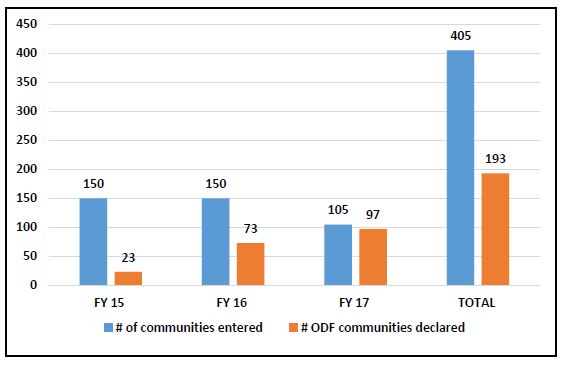
A key component of Ghana’s CLTS approach is for communities to construct their latrines and tippy taps with their own materials at their own expense. SPRING did not provide any materials or funds for construction. In the 405 communities where we worked, over 9,000 households built latrines, and over 8,000 had a tippy tap by their latrine (see figure 4). A total of 193 communities were declared ODF by the District Interagency Coordinating Committee on Sanitation (see figure 5). These results show that the CLTS process motivated communities to work towards improving their hygiene and health.
School WASH
To support our CLTS/WASH 1,000 activities, we also created interventions at schools in these communities. Schoolchildren are a powerful resource for creating change, able to encourage behavior changes among their peers and at home with their families. We trained 251 School Health Education Programme teachers, who in turn formed and mentored WASH/health clubs in 155 schools. The clubs participated in outreach activities at their schools, such as dramas, health talks, and handwashing demonstrations. Because traditional tippy taps, built with a plastic jug to hold the water, are difficult to use for large groups, we procured and installed large metal handwashing structures at 125 schools.
Figure 4. Household Latrines and Tippy Taps Constructed
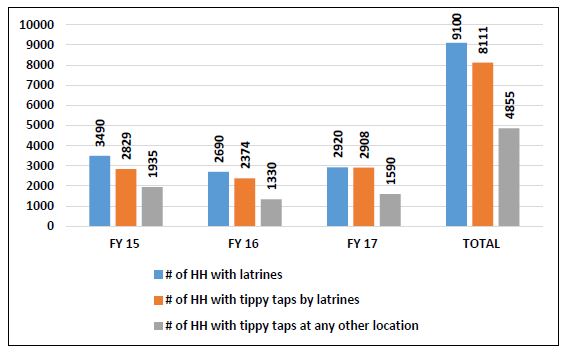
Figure 5. Number of Communities Achieving Open Defecation Free Status by Program Year

Agriculture
SPRING’s agriculture component offered another opportunity to engage with 1,000-day households by targeting family members who worked as farmers. Most of our work in agriculture focused on reducing exposure to aflatoxins in groundnuts, but also included communicating with farmers via short messaging services, introduction of other nutrient-rich crops, and a partnership with USAID and The Hershey Company to promote production of safe, healthy groundnuts.
Farmer Field Schools
To engage with groundnut farmers on agriculture practices, we implemented a farmer field school (FFS) approach. The FFS allowed community members to learn on-the-farm, with demonstrations of good agronomic practices that took place throughout the pre-harvest, harvest, and post-harvest seasons. The FFS were facilitated by agriculture extension agents (AEAs), who work under the Ministry of Food and Agriculture (MoFA) and received training from SPRING.
An FFS took place in each of our 405 communities. We developed an FFS curriculum that guides participants through seven modules covering groundnut growing practices. Groundnuts are a nutritious, widely-cultivated crop in northern Ghana. They are also highly susceptible to aflatoxins that are produced from molds that grow on improperly handled crops and that, when consumed, can cause serious health problems that inhibit the body’s ability to absorb nutrients. Because of their prevalence and susceptibility, groundnuts were a natural choice for our FFS interventions.
Supporting Women Farmers Through FFS Training
For its work with farmer field schools (FFS), SPRING recognized the need to adapt training to the needs of women farmers who make up a large part of the agricultural workforce. Training was offered in 60–90 minute segments, scheduled when most convenient to women, and used appropriate language and relatable examples. When working with pregnant women and mothers of children under the age of 2, SPRING used short, frequent engagements with trainees to maximize time and content.
One mother of five children, Mrs. Amina Woyom of Gushegu District, received FFS training along with 50 other farmers from her community to learn about good agronomic practices and post-harvest management. After applying her new knowledge, within the first year she was able to increase her groundnut yield from 123 kg/acre to 328 kg/acre.
She said, “Today I am the best woman farmer because I have adopted the best practices [that] the Agric.[culture] Officers taught us. People visit my farm to see what I am doing, which made me very proud. I know that by next year, many women will surprise SPRING and Department of Agriculture because they have seen the evidence in me.”
The curriculum guides participants through the growing year. It promotes good agronomic practices in pre-harvest activities (such as site selection, planting, and weeding), harvest, and post-harvest activities (such as drying and storage). Farmers discussed the possibility of aflatoxin contamination at different stages of cultivation, and what they could do to mitigate the risks. The curriculum also promotes our nutrition and WASH interventions by reinforcing messages around IYCF and the four key WASH behaviors.
By the end of the project, we had trained 274 AEAs to facilitate FFS, who in turn trained nearly 20,000 groundnut farmers. Of this number, 14,259 were women farmers; groundnuts are generally considered to be a women’s crop in Ghana. In addition to increasing awareness of the risks of aflatoxin contamination, the FFS also resulted in increased yield and better quality of groundnuts. In some groups, farmers reported that they had previously stopped growing nuts due to contamination and low yields, but were pleased to see that the good agronomic practices SPRING promoted helped improve their crops. In some cases, the increased yield and quality of groundnuts also led to improved income for farmers, who had more high-quality nuts to sell at the market.

Weather and Market Short Messaging Service
To help farmers have better access to information and weather and market prices in their area, we partnered with VOTO Mobile to send short messaging service (SMS) and voice messages to a cohort of SPRING-supported women farmers. Weather updates were delivered once per week, while market prices for crops and other agronomic information was delivered twice per week. VOTO Mobile also delivered nutrition messages. Over a six-month period, 4,542 farmers across our 15 districts received these messages. The information was delivered in local languages, include Dagbani, Gonja, Kusaal, Gruni, and Likpakpanl. Farmers who received these messages reported that the information was useful in planning their agricultural and market activities.
Nutrient-Rich Crop Cultivation
In an effort to combat micronutrient deficiencies, SPRING promoted the cultivation of orange-fleshed sweet potatoes (OFSP) and vitamin A-enriched maize. We worked with the Resiliency in Northern Ghana (RING) project and the Agriculture Technology Transfer (ATT) project, two other Feed the Future partners, to extend their work with these crops into SPRING-supported communities. We supplied 15 MTMSGs in two districts with vitamin A maize seeds for cultivation, and distributed over 20,000 OFSP vines to 80 MTMSGs in eight districts. Feed the Future partners also trained AEAs on the cultivation of these crops so that they could effectively train the MTMSGs. The farmers eagerly adopted these new crops and expressed an interest in continuing cultivation in subsequent growing seasons. We connected these groups with ATT and RING to ensure the MTMSGs received the needed support after SPRING closed.

Aflatoxin Research
We engaged in not only creating awareness on aflatoxin and supporting agronomic activities for its control but also conducting research activities to contribute more information on its implications for the value chain. In collaboration with Institute for Development Research Advocacy and Training and the University for Development Studies–Tamale, we conducted separate studies to examine the level of aflatoxin contamination existing in household stocks of groundnuts and aggregator stocks of maize and to assess whether there was an existing market premium for aflatoxin-safe groundnuts in our ZOI. The research findings show that there was no current market premium for aflatoxin-safe groundnuts, but there was a clear premium for clean, sorted, and graded groundnuts, which may be taken as proxy for aflatoxin-safe groundnuts. Additionally, household groundnut testing revealed a contamination rate of less than 9 percent overall, while the aggregator maize stocks had a contamination level around 25 percent. These results indicate that the problem of contamination may not be difficult to manage at the household level with concerted interventions such as the FFS approach. Our research results were shared at a national conference of Feed the Future stakeholders and are being processed for publication.
Public Private Partnership to Enhance the Groundnut Value Chain
SPRING believes that increasing the supply of aflatoxin-free groundnuts should be combined with increased demands for safe groundnuts. To this end, SPRING partnered with Project Peanut Butter to establish domestic manufacturing of safe and nutritious foods. We participated in a successful public-private partnership collaboration, culminating in a public event commemorating the launch of the groundnut-roasting equipment in Kumasi, Ghana in August 2017. We sourced, procured, and delivered the equipment as part of the partnership between USAID, the Hershey Company, and Project Peanut Butter, with the goal of providing safe, nutritious foods to children in Ghana. The use of the groundnut-roasting equipment will contribute to the groundnut value chain in Ghana, and help increase the incomes of Ghanaian groundnut farmers. The immediate use of the equipment, however, contributes to the current production of the groundnut-based nutritional supplement to schoolchildren, which is part of the Ghana School Feeding Program. This activity represents a potential market for domestically grown and safe groundnuts, such as those now produced by SPRING beneficiary farmers.

Social and Behavior Change Communication
Our social and behavior change communication (SBCC) strategy cut across the three sectors where we worked: nutrition, WASH, and agriculture. We defined key behaviors within these sectors to mitigate major causes of stunting. These behaviors included: increased consumption of animal source foods by young children; consistent consumption of frequent meals; clean play spaces for young children; improved handwashing and latrine use; and better agronomic, food storage, and preparation practices to reduce aflatoxins. The team used in-depth analysis to create a strategy that would address the motivation to take up new behaviors, capability of individuals and communities to sustain these behaviors, and opportunity to practices new behaviors. Knowing that our objectives of improving health and nutrition outcomes for 1,000-day households could not be achieved by service interventions alone, we created and used several SBCC materials to promote uptake of new behaviors. These materials included videos, radio programs, photo aids, and other resources.
Video
We produced several community videos for different sectors to use in sensitizing communities to good practices. By using local drama troupes, we were able to portray locations, people, and situations that would be familiar to our audiences. One of these was an advocacy video on stunting, meant to help community leaders understand what stunting is, why it is a problem, and how to fight it in their communities. The video, “When a King Has Good Counsellors, His Reign is Peaceful,” was screened among groups of mostly male leaders when SPRING first entered communities to work. It was produced in five languages spoken in our communities: Dagbani, Gonja, Kusaal, Gurune, and Likpakpanl.
We also produced a WASH 1,000 drama that draws attention to the four key WASH behaviors. The video was screened in 366 of our communities, and these screenings were later adopted as a standard part of the triggering phase of CLTS. Similar to this, we produced an aflatoxin awareness video, which was disseminated at community-wide screenings. This video serves as an additional tool for AEAs working in the community and was used to widen our agriculture reach beyond members of the FFS. Both the WASH 1,000 drama and the aflatoxin awareness video were produced in the five local languages mentioned above.
Finally, we created four short videos on IYCF that demonstrate key feeding practices that were difficult to explain during counseling. The videos show proper attachment during breastfeeding, positioning of the child during breastfeeding, meal diversity during complementary feeding, and a recipe for nutrient-rich mashed yam. These were loaded onto memory cards and distributed to nearly 1,300 health staff and CHVs, who put the videos on their mobile phones to use during counseling sessions. The videos help avoid the burden of physical demonstrations, which are often not possible during counseling sessions, while still helping caregivers learn best practices for feeding their children.
Radio
Household radio ownership is high in northern Ghana, even in rural areas, so SPRING decided to take advantage of the access to households radio provides. Our main radio project was a six-part serial radio drama called “Shrubs of Today Become Tomorrow’s Forest,” which promoted good IYCF practices targeting 1,000-day caregivers. The episodes were broadcast over a three-month period on eight local radio stations across the Northern and Upper East regions where we worked. This three-month broadcast happened twice, in 2016 and 2017. In addition to the radio broadcasts, we provided CHVs who facilitated MTMSGs with the episodes loaded onto memory cards. We purchased radio sets that worked with the memory cards for 300 MTMSGs, and the radio episodes were incorporated into their monthly meetings and discussions.
We also produced a two-part radio drama on aflatoxin control strategies. This drama was used to stimulate discussions during FFS. Similar to our other radio program, the drama was broadcast on eight radio stations operating in our implementation region. Both programs were produced in the five languages local to the area.

Photo Aids and Other Resources
To complement some of our technical resources, we created auxiliary illustrative job aids to improve communication of best practices between facilitators and audiences. This was especially important in our local context, since literacy rates are low in the communities where we worked. These resources included an aflatoxin management photo aid, used in FFS; a WASH 1,000 photo aid, used in the CLTS process; supplementary counseling cards for the IYCF curriculum used with MTMSGs; and a set of illustrative counseling cards that complement the discussion guide for FTFSGs. These photo aids and counseling cards helped foster discussion among groups and aided CHVs and other health workers in their work. These resources remain available to groups in Ghana and can be used in future interventions after the close of SPRING.
Social Protection Activities
Village Savings and Loan Associations
Because many households lack the resources to pay for health care, nutritious foods, or agricultural inputs, we implemented the village savings and loan association (VSLA) approach in 49 communities. Using existing MTMSGs, we formed a total of 49 VSLAs in the seven districts where we overlapped with the RING project, which was also using this intervention. After introducing the concept to the women, we provided them with operational kits that included a locked metal cash box, member cards, and a cash register to start accumulating savings and distributing loans. Over a month of implementation, the groups have accumulated a total of 107,342 Ghanaian cedis (about US$24,000) in savings. We received positive feedback on the program from participants. RING will continue to supervise the VSLAs after SPRING closes.
LEAP 1,000
The Livelihood Empowerment Against Poverty (LEAP) program, supported by USAID and UNICEF, is a cash transfer program run by the Government of Ghana to provide monetary support to poor and vulnerable households. Working with the Ministry of Gender, Children, and Social Protection, SPRING extended a qualification for LEAP assistance to 1,000-day households, creating a part of the program called LEAP 1,000. This extension targeted poor households with pregnant or lactating women and children under age 2 to receive cash assistance. The program helps raise spending levels and give households better access to healthcare, food, and shelter, improving the material and physical wellbeing of mothers and children. We aided the implementation by selecting 10 of our 15 districts to participate in the program, where stunting and poverty levels were highest. While not all of our communities received LEAP assistance, we co-implemented with LEAP 1,000 in 97 communities.
Best Practices, Challenges, and Recommendations
Best Practices
Through our program in Ghana, SPRING demonstrated that our two guiding practices were effective in promoting uptake of new behaviors and in decreasing rates of stunting:
- we implemented a multi-sectoral program with a variety of interventions in the same communities, and
- we used the 1,000-day household approach to target those interventions.
There is increasing evidence that multi-sectoral programs are effective in creating change, which our experience in Ghana supports. By introducing interventions across the nutrition, WASH, and agriculture into communities, we were able to reach the same communities with a variety of messaging platforms. We made relevant nutrition-specific and nutrition-sensitive programs that reached many community members in a variety of spaces, including at health facilities, at home, and on the farm. Working across sectors helped us saturate the community with positive messaging to achieve behavior change.
Within our multi-sectoral project, SPRING saw a need to focus our interventions on specific households to have the most impact. Acknowledging that people do not live their lives in silos or sectors, our hallmark 1,000-day household approach targeted the various needs of 1,000-day households across all of our interventions. Caregivers in 1,000-day households participated in mother-to-mother support groups, were trained in farmer field schools, and worked with water and sanitation management teams to build latrines at home. By focusing our activities to target mothers and children under 2 years of age, we were able to achieve a greater impact in reducing stunting and increasing uptake of behaviors, such as installing functional tippy taps in households and feeding children a minimum acceptable diet. Targeting 1,000-day households was especially impactful through our CLTS/WASH 1,000 approach, which saw a relatively quick adoption of new behaviors and achievement of ODF status in 193 communities.
Challenges and Recommendations
Despite the progress made towards reducing stunting, northern Ghana remains a vulnerable zone with persistent challenges and poor health indicators. We experienced a number of challenges over our three years of implementation that we hope will be addressed if future projects are to be successful. Our project was large, with many interventions across sectors, and implemented over a short period of time. Due to the size and breadth of coverage needed to influence activities according to district priorities and community comfort with our project, several of our programs ran without sufficient time to complete, including our quality improvement cycles and our work with VSLAs. The lack of health resources and commodities proved a limiting factor for some of our programming, and we were challenged by an insufficient investment in procurements and logistics. The scale of these issues was not well understood when our project began, and needs to be addressed in the future. There were also many other health projects or initiatives operating in northern Ghana that had similar goals, with little overlap in technical components and geographical areas, so it was difficult to coordinate programs and leverage experiences among implementers. While these challenges persist in Ghana, they did not prevent us from conducting our work effectively.
There are many lessons to be learned from SPRING’s experiences in Ghana. In addition to our overarching recommendation of multi-sectoral implementation and targeting of 1,000-day households to achieve impact, we offer the following recommendations:
- Dietary diversity can be better addressed in programming by combining communications with production of food. The farmer field school approach is an effective vehicle for reaching farmers and promoting dietary diversity.
- Production of nutrient-rich crops was not a large part of our program, but beneficiaries were enthusiastic about our small pilot projects with enriched maize and orange-fleshed sweet potatoes.
- Health services should focus on scaling up quality IYCF programming. Optimal IYCF promotion is key to preventing child malnutrition, and IYCF interventions should be a higher priority among health service providers.
- SPRING trained many technical staff in WASH, IYCF, anemia, and agriculture practices, and developed training and implementing resources for each of these sectors. These materials and staff should continue to be used, and the respective government institutions should scale up these resources so that they may be used country-wide.
- District ownership of interventions should be a high priority for future projects. District agencies play a crucial role in the delivery of services across sectors, and tapping into this role was essential to access the needed personnel and infrastructure to run our interventions. District buy-in was necessary to SPRING’s delivery of integrated programs and their embrace was our key to our success.

Conclusion
During our three years of implementation, SPRING/Ghana carried out a successful multi-sectoral program to improve nutrition within the 15 districts of the Upper East and Northern regions where we worked. By focusing on 1,000-day households, we were able to reduce stunting from 20.9 to 16.9 percent among children under 2 years of age and were also able to increase the prevalence of children in this age group receiving the minimum acceptable diet from 9.5 percent to 29.5 percent. SPRING also trained a total of 2,477 CHVs and 1,528 health staff from over 280 health facilities within our area of implementation on IYCF, helping to build capacity within the districts where we worked and ensure sustainability of the achievements reached during the life of our project.
To help ensure continuity of our approach and to disseminate important lessons learned, SPRING hosted learning events at the district levels throughout August 2017. In September 2017, SPRING hosted one final event at the national level in Tamale, chaired by the Regional Director of the Ghana Health Service for the Northern Region. This event gave us the opportunity to highlight the project’s achievements and offer recommendations to the Government of Ghana to sustain improvements seen under SPRING. District government staff, a community leader, and other project beneficiaries gave testimonials about the benefits of SPRING's multi-sectoral approach. One project beneficiary, the mother of a child under two, said, “Following SPRING’s advice, we have seen improvements in our lives. My children get sick less often, and we don’t have to go to the clinic as often.” At the closing, a vote of thanks acknowledged the contribution of USAID and the SPRING program for helping Ghana make strides in its goals to address malnutrition.
To view the annex, please download the full report above.
References
1 Ghana Statistical Service (GSS), Ghana Health Service (GHS), and ICF International. 2015. Ghana Demographic and Health Survey, 2014. Rockville, MD, USA: GSS, GHS, and ICF International.
2 Ghana Statistical Service (GSS), Ghana Health Service (GHS), and ICF International. 2015. Ghana Demographic and Health Survey, 2014. Rockville, MD, USA: GSS, GHS, and ICF International.










