Process Documentation Findings
Executive Summary

Anemia, a widespread public health problem, affects nearly 25 percent of the world’s population and undermines countries’ progress in health and economic development. Recognizing the scale and complexity of this problem, country governments and global agencies have reaffirmed their commitment to reduce anemia using an integrated multi-sector approach.
Since 2014, USAID SPRING project has supported the Ministry of Health and Sanitation (MOHS) and stakeholders working to reduce anemia in Sierra Leone to strengthen multi-sectoral anemia programming at the national level. This is a country-led process to create evidence-based and context-specific strategies to reduce anemia.
The National Anemia Working Group (NAWG), a multi-sectoral anemia coordination platform, was constituted in 2016. The NAWG, chaired by the MOHS and comprising national stakeholders working to reduce anemia, provides a platform for convening diverse sectors and partners to define and advance Sierra Leone’s anemia priorities.
This report identifies challenges and successes of establishing a multi-sectoral anemia platform in Sierra Leone, explores key factors that led to the outcomes, and identifies potential areas for future progress in reducing anemia. Findings are based on data from two rounds of semi-structured qualitative interviews conducted by SPRING staff with key informants and all NAWG members and observations made by technical assistance providers.
SPRING gathered informants’ perspectives about the NAWG’s function and strategic direction, multi-sectoral coordination and collaboration, anemia strategy development, and sustainability of anemia efforts. The key findings emerged in three main areas: having data as a critical agenda setter; establishing a national anemia working group, and developing and implementing the anemia prevention and control strategy.
Data
- Equipped with rich and reliable data, stakeholders in Sierra Leone had evidence to help guide efforts and decision-making.
Establishing a National Anemia Working Group
- The NAWG must have high-level endorsements to engage stakeholders in multi-sectoral work.
- The deliberations during the NAWG meeting were contingent on the active participation of the stakeholders. Meeting organization was critically dependent on staff dedicated to the logistics for NAWG meetings. Robust communication is essential for continued member engagement.
- Development of a Google group provided a platform for sharing resources with current and potential NAWG members and reduced difficulties with changing membership due to high turnover.
- NAWG members are positive about cross-sector collaboration for knowledge sharing, networking, and relationship building.
Development and implementation of the Sierra Leone Anemia Prevention and Control Strategy
- Inadequate funding is a potential barrier to sustaining anemia efforts and implementing the anemia strategy.
- Community and district-level engagement is an important component for linking to national anemia efforts and requires targeted efforts.
The report concludes with suggestions and considerations for the continuation of the NAWG, dissemination and implementation of the anemia strategy, further engagement of district-level stakeholders, and efforts to advocate for prioritization of anemia at the national and district levels.
Introduction
Anemia, a widespread public health problem, affects nearly 25 percent of the world’s population. Currently, few countries are on track to meet the World Health Assembly (WHA) nutrition target of reducing anemia by 50 percent by 2025. Women and children in resource-limited settings bear the highest burden of anemia-related morbidity and mortality. Children with anemia have long-term, irrevocable cognitive and developmental delays, and decreased worker productivity as adults (Walker et al. 2007). Iron-deficiency anemia contributes to adverse birth outcomes and is the underlying cause of 115,000 maternal and 591,000 perinatal deaths each year (Stoltzfus et al. 2004). In recognition of the scale of this problem, global and national commitment to addressing anemia continues to rise, shown by the specific focus on anemia in WHA’s six global targets to improve nutrition (WHO 2017).
The causes of anemia are complex and overlapping and include nutritional deficiencies, infections, inflammatory conditions, and genetic disorders (Balarajan et al. 2011). Because of anemia’s multiple causes, interventions that involve various stakeholders and collaboration across sectors—including agriculture, education, health, communication, gender, finance, and water, sanitation, and hygiene—are critical for effective prevention and control efforts.
Momentum for multi-sectoral and integrated approaches to nutrition and a revived focus on anemia are growing globally. Reducing anemia among vulnerable populations is critical to improve nutrition outcomes and to have a positive impact on maternal and child health and survival. The Government of Sierra Leone, with support from SPRING, has worked with national sectors and stakeholders to strengthen multi-sectoral programming at the national level and has created a comprehensive strategy to address anemia.
This report documents Sierra Leone’s anemia programming experience between April 2014 and December 2017. It uses data from qualitative interviews and participatory observation to uncover critical factors including enablers and barriers for strengthening multi-sectoral anemia coordination for country stakeholders.
Overview of the Multi-sectoral Anemia Platform in Sierra Leone
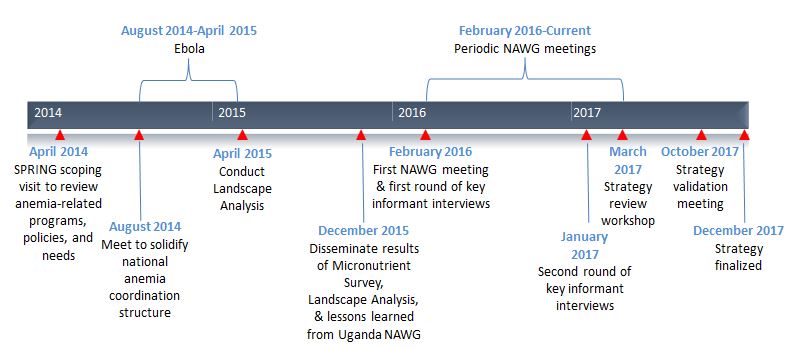
The multi-sectoral initiative to reduce anemia in Sierra Leone, with SPRING support, spanned four years: 2014 to 2017 (see Figure 1). The effort originated from a Ministry of Health and Sanitation (MOHS) request for SPRING’s technical support to conduct an analysis of the anemia landscape. Findings highlighted the high prevalence of anemia and surprisingly low prevalence of iron deficiency. They also underlined gaps in the coverage of anemia-related interventions. These findings prompted in-country stakeholders to establish the multi-sectoral National Anemia Working Group (NAWG) stemming from Scaling Up Nutrition (SUN) efforts. The NAWG is chaired by the Food and Nutrition Directorate, with Helen Keller International acting as secretariat and SPRING providing on-going technical assistance. The NAWG comprises representatives from stakeholders across sectors including agriculture, health, water and sanitation, communication, gender, and finance. The NAWG is responsible for coordinating, planning, implementing, and monitoring in-country anemia initiatives.
Figure 1. Timeline for National Anemia Efforts in Sierra Leone
Process Documentation: Rationale
Policy-making is complex and dynamic. As countries develop policies and plan to strengthen national nutrition programming, it is critical to understand the process they undertake with respect to commitment, agenda setting, policy formulation, and implementation (Pelletier et al. 2012). Documentation of the process, which identifies key challenges and enabling factors faced by policy makers and implementers, helps countries plan for and improve upon policy formulation and implementation. The aim of this process documentation is to identify challenges and successes of establishing a multi-sectoral anemia platform in Sierra Leone, analyze the key factors that led to outcomes, and identify potential areas for making improvements to the process.
Methods
SPRING used a qualitative longitudinal case study methodology that included in-depth interviews with key informants and participant observations by SPRING staff, who conducted two rounds of semi-structured qualitative interviews. Round one was in February 2016, shortly after the newly established NAWG’s first meeting; it included 14 key informants. Round two, conducted one year later in January 2017, included 12 key informants.
The key informants, all members of the NAWG, were selected to represent a range of sectors/institutions and different levels of involvement. The interviews gathered informants’ perspectives about the NAWG, including function and strategic direction, multi-sectoral coordination and collaboration, anemia strategy development, and sustainability of anemia efforts. SPRING staff members transcribed interview recordings and analyzed each interview for a priori and emerging themes.1 They also reviewed key documents to understand the background, context, and progress of NAWG activities. These documents included anemia stakeholder meeting workshop notes and the Anemia Prevention and Control Strategy. In this report, key findings are organized by steps in the anemia platform-building process.
Key Findings
Data: A Critical Agenda Setter
In Sierra Leone, findings from the anemia landscape analysis were central to engaging stakeholders in NAWG efforts and had a key role in steering its composition, structure, and focus. The anemia landscape analysis collected data from sources including the micronutrient survey, Demographic and Health Survey, and post-event coverage surveys, as well as a literature review and discussion about the current policy environment and existing coordination platforms with in-country partners.
Everybody previously would have said ‘iron,’ and now people are realizing it’s not iron; …it’s WASH, and it’s malaria, and it’s genetics, and it’s perhaps something else as well.
Findings showed anemia is a severe public health problem in Sierra Leone. Prevalence in children under five and women of reproductive age is 76 percent and 45 percent respectively, with little or no improvement since 2008. Results from the micronutrient survey made the anemia landscape analysis particularly useful by providing nationally representative data about the prevalence of risk factors. Surprisingly, iron deficiency was not a main driver of anemia, as prevalence in Sierra Leone is low. Instead, the survey highlighted factors such as infection (especially malaria, respiratory tract, and diarrhea), general inflammation, and potentially genetic blood disorders as key contributors to anemia. This, in turn, revealed a mismatch between the major contributors to anemia and the interventions that were in place to address it, with discrepancies in program coverage. This rich and reliable data gave stakeholders evidence to guide efforts and decision-making.
Establishing a National Anemia Working Group
The NAWG was established shortly following the dissemination of the anemia landscape analysis results. The following components were essential to its establishment:
The directors of Food and Nutrition have been the driving force and have been involved in every working group meeting.
We keep the direct communication going. That is also resource-bound because it’s really expensive calling people up all the time…. It takes a lot of work even when we have partners… we have to really go out of our way— email, call, ‘please this is important.
- High-level endorsement was an important first step to bring attention to and build momentum about anemia in Sierra Leone. From the outset, the working group benefitted from strong, dedicated leadership and endorsement from the MOHS. This heavily influenced willingness of stakeholders to engage in NAWG efforts. Findings from the landscape analysis made stakeholders aware of the need to prioritize actions addressing anemia by not only MOHS, but a range of sectors and partners.
- Using the Scaling Up Nutrition (SUN) coordination platform was essential for quick startup and integration with existing structures. The NAWG was established strategically under SUN, which, starting in 2012, provided structure for coordinating multi-sectoral efforts for improved nutrition in Sierra Leone. SUN had nominated sectoral government representatives to participate in activities related to nutrition, which was a useful starting point for mobilizing stakeholders to participate in NAWG efforts. In addition, the SUN structure allowed the NAWG to avoid duplicating efforts and meeting content of other nutrition-related working groups. The overarching SUN coordination helped ensure that meeting schedules of various working groups did not overlap to minimize occasions when competing priorities prevented participation in NAWG meetings.
- A robust communication and follow-up strategy was key for higher turnout and continued member engagement. Although costly and time-consuming, targeted reminder phone calls to communicate meeting times and agendas and follow-up emails to share minutes and presentations motivated NAWG members. Consistent communication and follow-up were especially important in the Sierra Leonean context, where partner staff turnover was exceptionally high after the end of the Ebola outbreak. NAWG meeting organizers learned quickly that the list of attendees needed consistent updating to reflect the most recent stakeholders. A Google group of NAWG member, attendees, and persons expressing interest and expertise was regularly updated so that NAWG meeting minutes, reports, Youtube links, and other relevant information could be disseminated efficiently.
Collaboration between NAWG sectors
Coordinating stakeholders across sectors and departments was a central component of Sierra Leone’s anemia platform. This multi-sectoral engagement is an opportunity for actors previously working independently of one another to collaborate in pursuit of the overarching goal of anemia reduction in Sierra Leone. The NAWG has become an active and participatory platform to coordinate anemia efforts. Between January 2015 and August 2017, the NAWG held 10 periodic meetings as well as sub-group meetings for strategy development and review. Themes from stakeholder discussions involving cross-sector collaboration were:
When you talked about anemia being a multi-sectoral problem, nobody quite got it, until we realized, ‘hold on a minute, anemia isn’t due to nutrition…the nutritional aspects are a minor part of the problem.’ So for all this responsibility to be on the shoulders of one person at the Ministry of Health doesn’t make sense…she can’t move the indices herself.
The biggest weakness throughout the country is WASH. That’s why we had Ebola. If we could solve WASH, then we could solve lots of things.”
- NAWG’s role as a platform for learning and information-sharing keeps members motivated. Many key informants described NAWG meetings as learning sessions that expanded their knowledge base and motivated them to continue attending and participating in meetings. Initially, NAWG targeted individuals with specific technical backgrounds, which hindered representation from the range of sectors needed for anemia reduction. As a result, NAWG cast a wide net to recruit technical and non-technical members. Similarly, the content presented at initial meetings was largely technical, which deterred some stakeholders who “weren’t speaking the same language” from continuing to participate. NAWG leadership learned the importance of balancing the perspectives of diverse sectors and stakeholders to engage a truly multi-sectoral working group. For continued engagement, one key informant suggested providing opportunities for members to present how their sector, department, or organization could contribute to NAWG efforts.
- Cross-sector collaboration was a priority for NAWG members once they realized that despite initial beliefs, iron deficiency has a relatively minimal role in anemia. The NAWG helped develop cross-sector working relationships and strengthened key partnerships. For instance, many key informants stressed the important role of the water, sanitation, and hygiene (WASH) sector in anemia reduction, given the role of infections and inflammation in causing anemia and the low coverage of WASH interventions throughout Sierra Leone. Despite members’ appreciation and enthusiasm for a multi-sectoral approach, continued engagement and regular attendance of non-health members has been challenging, in part due to the still-prevailing perception that the Ministry of Health and health-related nongovernmental organizations have “mandates” to lead anemia reduction efforts, while other sectors have supporting roles only.
- The NAWG was an opportunity to identify gaps in program coverage and avoid duplication of efforts across sectors and stakeholders to maximize investments. As key informants explained, NAWG meetings were an occasion for members to build personal relationships, share information about their anemia-related activities, and explore options for how they could better coordinate efforts. Key informants also mentioned coordination across partners and between national, district, and chiefdom levels as an essential component of improved programming. While many mentioned the need for ongoing coordination to avoid duplication of efforts, some went further to suggest integration of some services using NAWG’s platform. For instance, one key informant stressed the importance of reaching pregnant women—a high-risk group for anemia—through high-quality comprehensive antenatal care that includes iron and folic acid supplementation, intermittent preventive treatment in pregnancy and bed nets for malaria prevention, and deworming.
Development and Implementation of the Sierra Leone Anemia Prevention and Control Strategy
Shortly after its establishment, the NAWG embarked on developing a comprehensive multi-sectoral anemia strategy. Key informants noted that each sector contributed significantly throughout the development process, which fostered cross-sectoral ownership. Key informant lessons from strategy development and next steps for effective implementation included:
Not rushing has…given us time to realize there is other stuff we needed to put in [the strategy], like the social protection and the female education, which we really hadn’t give much thought to at the beginning.
[We] don’t want to leave it at the strategy stage; [we] want to go beyond that and have an action plan so everyone knows what they’re doing and how they’re doing it, and have targets and work toward meeting those targets.
Last year was about getting people together, getting the idea of how anemia is linked to malaria, to HIV, to different sicknesses, so now we think people have some idea about these links, so now it’ll be about actions…I’ll say one of the great challenges is finance. So, I think if we get finance sorted out, it’ll be ok.
- Sectoral involvement was essential to develop an effective and non-duplicative strategy. NAWG members had ample time to contribute, review, and revise strategy content related to their work. The drafting process was slow, which gave contributors sufficient time to include all key stakeholders. After compiling a first draft of the strategy, the NAWG organized a one-day cross-sector review meeting. During this meeting, members broke into six groups to tackle each of the outlined objectives in the strategy and re-assess the listed priority actions to ensure that they reflected current context and evidence. Low-priority items were cut from the strategy and missing items were added. Sectoral input was not only key to fostering ownership of the strategy, but also to ensuring that plans for implementation were actionable.
- Political commitment and widespread dissemination of strategy are next steps. Key informants expressed that an effective strategy launch would entail a large dissemination event with attendance from top government officials and a keynote speaker to provide context and introduce the document. NAWG members agreed that after the strategy is disseminated, meeting semi-annually to present new information and innovations will be sufficient, as long as individual sectors continue to make progress.
- Moving forward, adequate funding is critical to implementing the strategy. While the strategy is a multi-sectoral document, almost all key informants emphasized that implementation would be done within individual sectors, with support and coordination from other sectors and integration of services as appropriate. For this to work, strategy activities will need to be integrated with the implementation framework of each sector, aligning with annual work plans and budgets, and monitoring of indicators. Key informants expressed the challenge of properly financing these activities, and stressed the importance of involving representatives from the finance department in the NAWG at the strategy development stage so they would have a better appreciation of anemia and anemia reduction efforts, and be more likely to allocate sufficient funding.
- Key informants cited district-and community-level involvement as a necessity for successful strategy implementation. NAWG members echoed the importance of raising awareness about anemia and engaging district-and community-level stakeholders in anemia programming. Key informants mentioned the success of such efforts during the Ebola outbreak, which included channeling messages through community leaders, religious coalitions, traditional healers, and women’s networks, as well as using mass media communication strategies for broad reach. NAWG members also suggested that input from district and community stakeholders was key to ensuring that the strategy was appropriate for the Sierra Leone context. NAWG leaders made efforts to solicit participation from these stakeholders, especially during the strategy workshop and validation meeting.
Recommendations for Future Progress
Recommendations that emerged from the findings of the qualitative research fall into four areas: the NAWG, the anemia strategy, district-level engagement, and advocacy.
NAWG
- Determine ownership of anemia coordination efforts at the national level to sustain the NAWG after the SPRING partnership ends.
- Because national-level working group membership overlaps, consider retaining the NAWG as a sub-group of SUN, meeting bi-annually.
- Share information, updates, and resources with selected regional and district officials so that implementation-level staff have the information they need.
- Establish a mechanism for all sectors and districts to report anemia activity implementation progress. This will aid monitoring and identification areas needing support.
Anemia Strategy
- Disseminate the anemia strategy at the national level, across all government sectors and partners. Implementing partners at the regional and district levels should consider disseminating the strategies at the different levels.
- Integrate strategy actions into sectoral work plans and budgets, and ensure actions are supported by or harmonized with partner activities.
- During the next eight years of implementation, government sectors can use the indicators and the targets in the anemia strategy to track progress. Use the strategy’s monitoring and evaluation framework to assess progress and determine how sectors will report updates and progress.
- Explore integration of activities across sectors. This might include strengthening platforms to co-deliver anemia-related interventions, such as deworming and nutrition/hygiene education in schools.
- During the eight years of the anemia strategy, consider advocating for the collection of better data at the national level, integrating anemia-related data into national surveys, and determining the frequency of national-level surveys that collect micronutrient and anemia-related data.
District-Level Engagement
- Invite district-level stakeholders to future NAWG meetings and provide support for them to attend as needed, for example, providing funds for transportation costs or holding meetings outside of Freetown.
- After the anemia strategy is disseminated at the district level, determine how prioritized activities will be implemented and monitored, and align activities with the annual district planning cycles.
- Determine whether a local platform can link with the NAWG to coordinate anemia efforts across levels to help ensure sustainability.
- If resources are limited, consider prioritizing districts with the highest prevalence of anemia for program implementation.
- Explore options to harmonize district-level activities with partner-driven implementation of anemia-related interventions.
Advocacy
- Consider forming an advocacy technical group within the working group or use existing platforms to advocate for integrating anemia into sectoral work plans or budgets.
- Use the anemia strategy to develop plans for how to advocate to different audiences at the national, district, and community levels.
- Use lessons from successful high-coverage communications campaigns to ensure that everyone knows about anemia. Highlight the consequences of and gains related to preventing and treating anemia in messages targeted to various audiences.
- Consider using “anemia champions” (i.e., opinion, religious, local government leaders) for advocacy and to encourage community members to demand and use anemia-related services.
To view the annex, please download the full report above.
Footnotes
1 Quotations in this report are excerpted from the interviews with NAWG members.
References
Balarajan, Yarlini, Usha Ramakrishnan, Emre Ozaltin, Anuraj H. Shankar, and S. V. Subramanian. 2011. “Anemia in Low Income and Middle-Income Countries.” The Lancet 378 (9809):2123–35.
Pelletier, D. L., E. A. Frongillo, S. Gervais, L. Hoey, P. Menon, T. Ngo, R. J. Stoltzfus, A. M. S. Ahmed, and T. Ahmed. 2012. “Nutrition agenda setting, policy formulation and implementation: lessons from the Mainstreaming Nutrition Initiative.” Health Policy and Planning 27:19–31.
Stoltzfus, Rebecca J., Luke Mullany, and Robert E. Black. 2004. “Iron Deficiency Anaemia.” In Comparative Quantification of Health Risks: Global and Regional Burden of Disease Attributable to Selected Major Risk Factors, edited by Majid Ezzati, Alan D. Lopez, Anthony Rodgers, and Christopher J. L. Murray.,163–209. Geneva: WHO
United States Agency for International Development (USAID). 2014. “USAID Multi-Sectoral Nutrition Strategy 2014–2025.” http://www.usaid.gov/nutrition-strategy.
Walker, S. P., T. D. Wachs, J. M. Gardner, B. Lozoff, G. A. Wasserman, E. Pollitt, and J. Carter. 2007. “Child development: risk factors for adverse outcomes in developing countries.” The Lancet 369 (9556):145–157.
World Health Organization (WHO). 2014. “Global Targets 2025.” http://www.who.int/nutrition/global-target2025/en/.







